

Nature of Cardiac Rehabilitation Around the Globe
- PMID: 31517262
- PMCID: PMC6733999
- DOI: 10.1016/j.eclinm.2019.06.006
Nature of Cardiac Rehabilitation Around the Globe
Abstract
Background: Cardiac rehabilitation (CR) is a clinically-effective but complex model of care. The purpose of this study was to characterize the nature of CR programs around the world, in relation to guideline recommendations, and compare this by World Health Organization (WHO) region.
Methods: In this cross-sectional study, a piloted survey was administered online to CR programs globally. Cardiac associations and local champions facilitated program identification. Quality (benchmark of ≥ 75% of programs in a given country meeting each of 20 indicators) was ranked. Results were compared by WHO region using generalized linear mixed models.
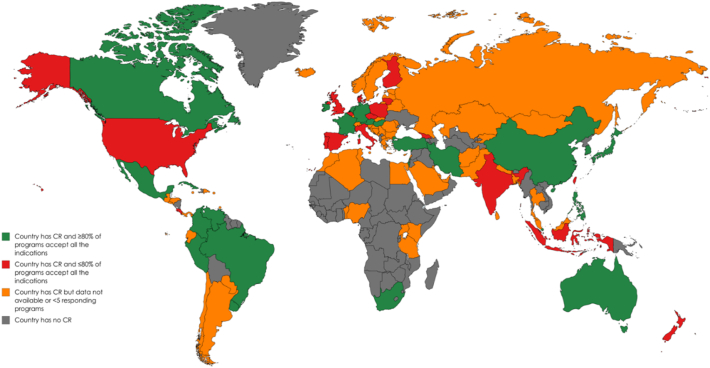
Findings: 111/203 (54.7%) countries in the world offer CR; data were collected in 93 (83.8%; N = 1082 surveys, 32.1% program response rate). The most commonly-accepted indications were: myocardial infarction (n = 832, 97.4%), percutaneous coronary intervention (n = 820, 96.1%; 0.10), and coronary artery bypass surgery (n = 817, 95.8%). Most programs were led by physicians (n = 680; 69.1%). The most common CR providers (mean = 5.9 ± 2.8/program) were: nurses (n = 816, 88.1%; low in Africa, p < 0.001), dietitians (n = 739, 80.2%), and physiotherapists (n = 733, 79.3%). The most commonly-offered core components (mean = 8.7 ± 1.9 program) were: initial assessment (n = 939, 98.8%; most commonly for hypertension, tobacco, and physical inactivity), risk factor management (n = 928, 98.2%), patient education (n = 895, 96.9%), and exercise (n = 898, 94.3%; lower in Western Pacific, p < 0.01). All regions met ≥ 16/20 quality indicators, but quality was < 75% for tobacco cessation and return-to-work counseling (lower in Americas, p = < 0.05).
Interpretation: This first-ever survey of CR around the globe suggests CR quality is high. However, there is significant regional variation, which could impact patient outcomes.
Keywords: Cardiac rehabilitation; Global health; Health services; Nature; Preventive cardiology; Survey.
Conflict of interest statement
Dr. Derman reports some financial activities that were outside the submitted work (i.e., grants from International Olympic and Paralympic Committees, as well as personal fees from 2 advisory boards). All other authors declare no financial or personal interests related to the work.
Figures
References
-
- Anderson L., Oldridge N., Thompson D.R. Exercise-based cardiac rehabilitation for coronary heart disease. J Am Coll Cardiol. 2016;67:1–12. - PubMed
-
- Thomas R.J., King M., Lui K. AACVPR/ACC/AHA 2007 performance measures on cardiac rehabilitation for referral to and delivery of cardiac rehabilitation/secondary prevention services. J Am Coll Cardiol. 2007;50:1400–1433. - PubMed
-
- Woodruffe S., Neubeck L., Clark R.A. Australian Cardiovascular Health and Rehabilitation Association (ACRA) core components of cardiovascular disease secondary prevention and cardiac rehabilitation 2014. Hear Lung Circ. 2015;24:430–441. - PubMed
-
- Grace S.L., Poirier P., Norris C.M. Pan-Canadian development of cardiac rehabilitation and secondary prevention quality indicators. Can J Cardiol. 2014;30:945–948. - PubMed
-
- Piepoli M.F., Corra U., Adamopoulos S. Secondary prevention in the clinical management of patients with cardiovascular diseases. Eur J Prev Cardiol. 2014;21:664–681. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
