

Association of the US President's Emergency Plan for AIDS Relief's Funding With Prevention of Mother-to-Child Transmission of HIV in Kenya
- PMID: 31517966
- PMCID: PMC6745052
- DOI: 10.1001/jamanetworkopen.2019.11318
Association of the US President's Emergency Plan for AIDS Relief's Funding With Prevention of Mother-to-Child Transmission of HIV in Kenya
Abstract
Importance: From 2004 to 2014, the US President's Emergency Plan for AIDS Relief (PEPFAR) invested more than $248 000 000 in the prevention of mother-to-child transmission (PMTCT) of HIV in Kenya. Concurrently, child mortality in Kenya decreased by half.
Objective: To identify the extent to which the decrease in child mortality in Kenya is associated with PEPFAR funding for PMTCT of HIV.
Design, setting, and participants: This population-based survey study conducted in Kenya estimated the association between annual per capita PEPFAR funding for PMTCT (annual PCF) and cumulative per capita PEPFAR funding for PMTCT (cumulative PCF), extracted using 2004-2014 country operational reports as well as individual-level health outcomes, extracted from the 2003, 2008-2009, and 2014 Kenya Demographic and Health Surveys and the 2007 and 2012 Kenya AIDS Indicator Surveys. The study included children of female respondents to the 2003, 2008-2009, and 2014 Kenya Demographic and Health Surveys who were born 1 to 60 months (for neonatal mortality) or 12 to 60 months (for infant mortality) before the survey, as well as female respondents who had recently given birth and reported on HIV testing during antenatal care (ANC) during the 2007-2014 surveys. Results were adjusted for year, province, and survey respondent characteristics. Statistical analysis was performed from July 8, 2016, to December 10, 2018.
Main outcomes and measures: Neonatal mortality was defined as death within the first month of life and infant mortality was defined as death within the first year of life. HIV testing during ANC was defined as receiving counseling on PMTCT, undergoing an HIV test, and receiving test results during ANC.
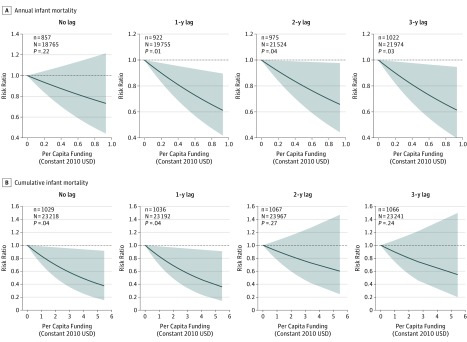
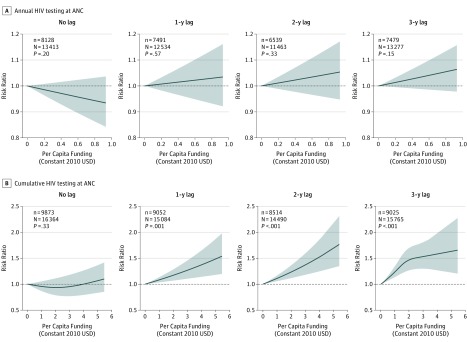
Results: The analysis included 33 181 neonates (16 870 boys), 26 876 infants (13 679 boys), and 20 775 mothers (mean [SD] age, 28.0 [6.7] years). PEPFAR funding was not associated with neonatal mortality. A $0.33 increase in annual PCF, corresponding to the difference between the 75th and 25th (interquartile range) percentiles of funding, was significantly associated with a 16% (95% CI, 4%-27%) reduction in infant mortality after a 1-year lag. A 14% to 16% reduction persisted after 2- and 3-year lags, and comparable reductions were observed for unlagged and 1-year lagged cumulative PCF. An increase of 1 interquartile range in cumulative PCF was associated with a 7% (95% CI, 3%-11%) increase in HIV testing during ANC, which intensified with subsequent lags. Between 2004 and 2014, sustained funding levels of $0.33 annual PCF could have averted 118 039 to 273 924 infant deaths.
Conclusions and relevance: Evidence from publicly available data suggests that PEPFAR's PMTCT funding was associated with a reduction in infant mortality and an increase in HIV testing during ANC in Kenya. The full outcome of funding may not be realized until several years after allocation.
Conflict of interest statement
Figures
References
-
- Measure Evaluation Hill K, Cheluget B, Curtix S, Bicego G, Mahy M. HIV and increases in childhood mortality in Kenya in the late 1980s to the mid-1990s. https://www.measureevaluation.org/resources/publications/sr-04-26. Accessed March 24, 2017.
-
- Kenya National AIDS and STI Control Programme (NASCOP) Kenya AIDS Indicator Survey 2012: Final Report. Nairobi, Kenya: NASCOP; 2014.
-
- Office of US Global AIDS Coordinator. PEPFAR Panorama Spotlight. https://data.pepfar.gov/dashboards. Accessed November 25, 2016.
-
- Kenya National Bureau of Statistics, Kenya Ministry of Health, Kenya National AIDS Control Council, Kenya Medical Research Institute, Kenya National Council for Population Development Kenya Demographic and Health Survey 2014: Final Report. Rockville, MD: Kenya National Bureau of Statistics, Ministry of Health, National AIDS Control Council, Kenya Medical Research Institute, National Council for Population Development, DHS Program, ICF International; 2015.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
