

Bile duct involvement by hepatocellular carcinoma: A rare occurrence and poor prognostic indicator in bile duct brushing samples
- PMID: 31518056
- PMCID: PMC7482131
- DOI: 10.1002/cncy.22185
Bile duct involvement by hepatocellular carcinoma: A rare occurrence and poor prognostic indicator in bile duct brushing samples
Abstract
Background: Hepatocellular carcinoma (HCC) rarely involves the biliary tree and may be inadvertently sampled on bile duct brushings (BDBs).
Methods: The pathology archives of 5 institutions were searched for BDBs with HCC involvement.
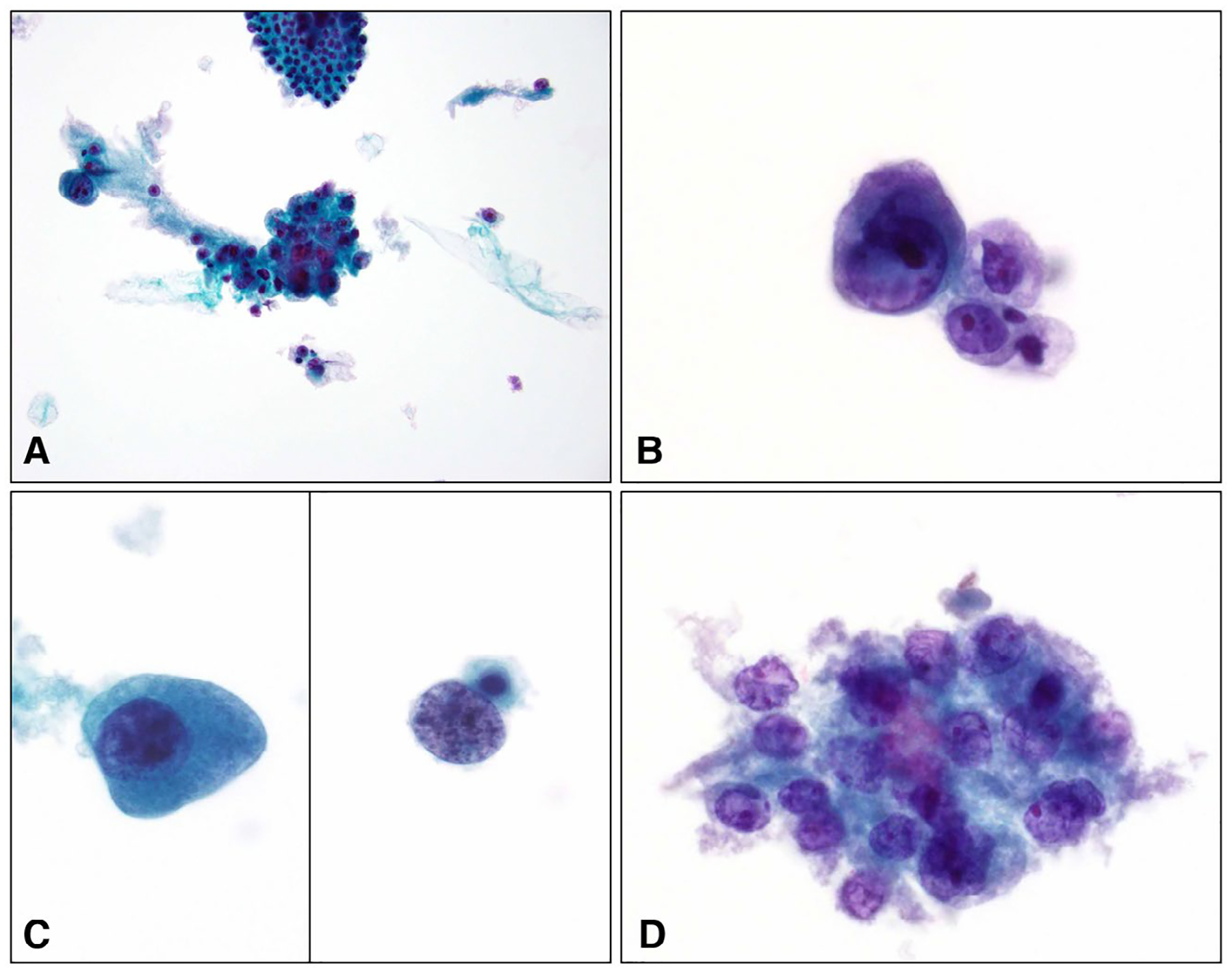
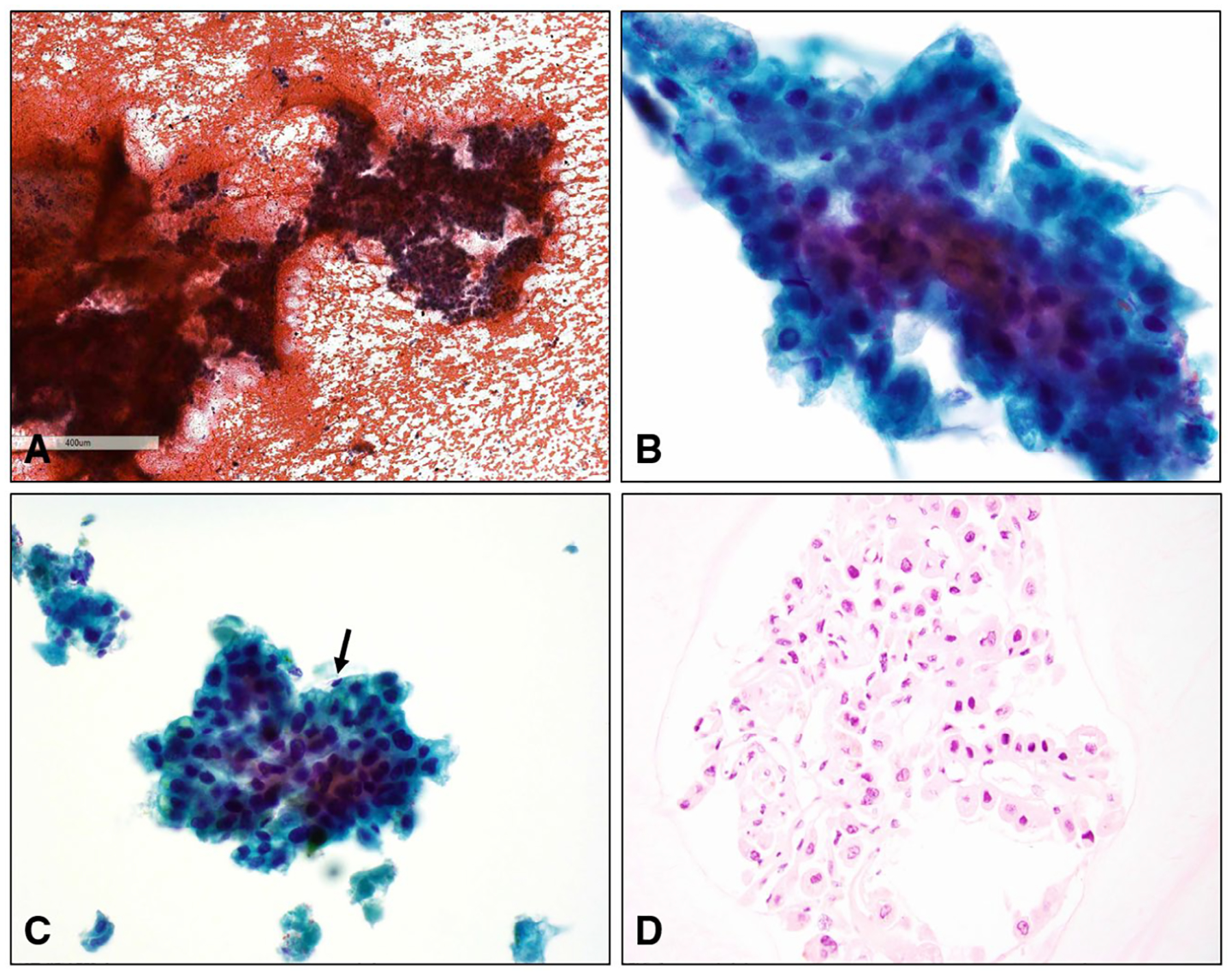
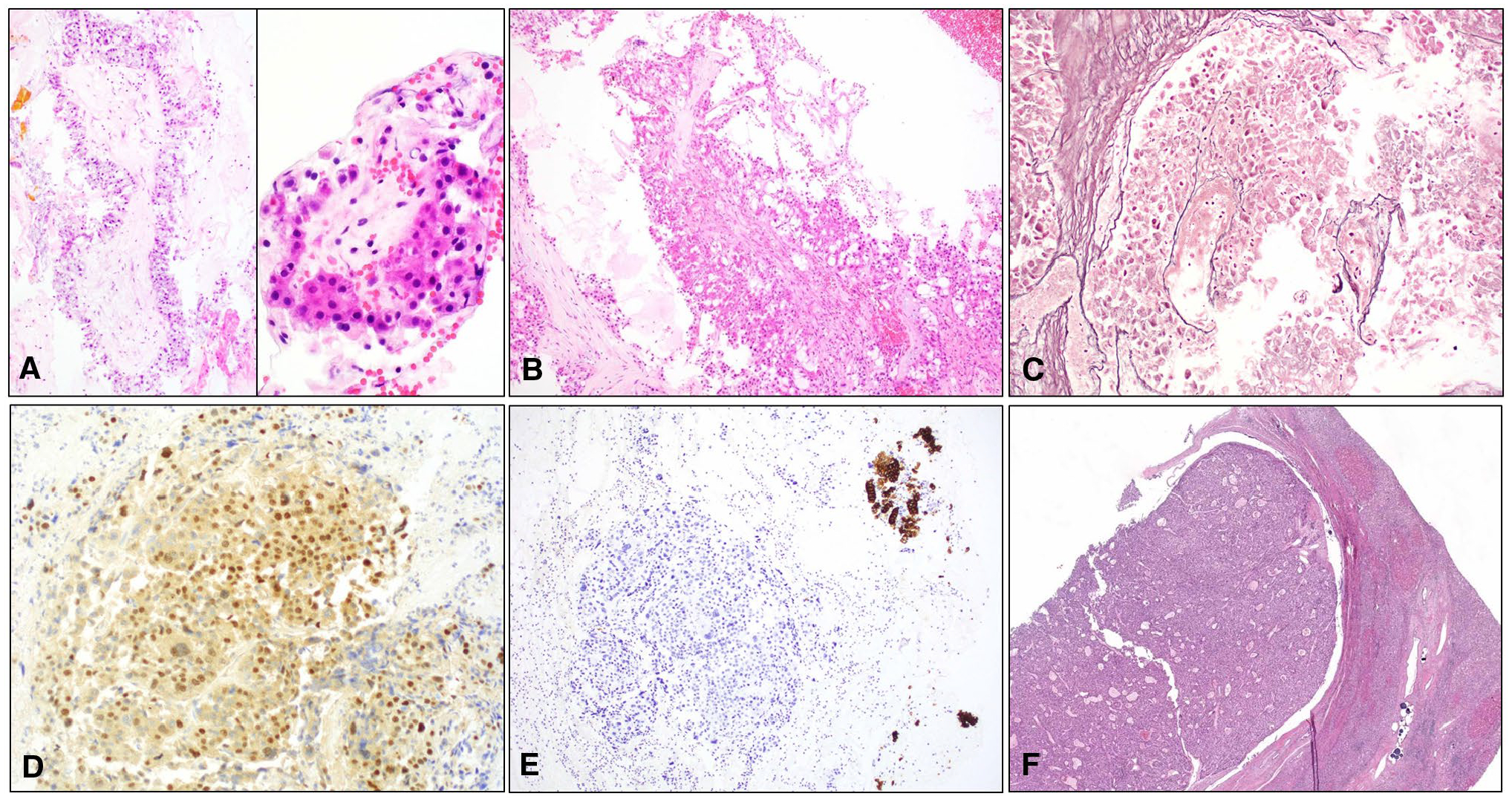
Results: A total of 17 BDBs from 14 patients were obtained. There was a male:female ratio of 6:1; the median age of the patients was 59.5 years (range, 22-80 years). The median hepatic tumor size was 6.2 cm (range, 2.2-13.0 cm). HCC risk factors included viral hepatitis (5 patients), cirrhosis (5 patients), hemochromatosis (1 patient), and alcoholic steatohepatitis (1 patient). Jaundice with elevated bilirubin, liver enzymes, and α-fetoprotein was common. Endoscopic retrograde cholangiopancreatography demonstrated bile duct dilatation, polypoid intraductal masses (5 samples), clots/debris (2 samples), or strictures (4 samples). All BDBs had single and clustered large cells with naked atypical nuclei, granular cytoplasm, high nuclear/cytoplasmic ratios, and nuclei with prominent macronucleoli. Less common findings included clear/microvesicular cytoplasm (35%), papillae (29%), and anisonucleosis (35%). Classic HCC features (widened trabeculae [35%], endothelial wrapping [24%], multinucleation [24%], and cytoplasmic bile pigment [35%]) were uncommon. A total of 11 BDBs were diagnosed as malignant (10 with HCC and 1 with cholangiocarcinoma), 2 were diagnosed as atypical, and 1 BDB was diagnosed as negative; approximately two-thirds were found to have polysomy on fluorescence in situ hybridization. Approximately 71% of patients died of disease at a median of 3.5 months.
Conclusions: HCC may extend into the intrahepatic and/or extrahepatic biliary tree, causing masses and/or strictures that may be sampled on BDB. Although cytologically malignant, the classic features of HCC are uncommon, which can cause misdiagnosis. Cytopathologists should be mindful of this differential when evaluating BDBs, particularly when concomitant liver masses and/or HCC risk factors are present. Because of the associated high mortality and rapid rate of death, its presence should be conveyed clearly in pathology reports.
Keywords: bile duct; brushing; carcinoma; hepatocellular.
© 2019 American Cancer Society.
Conflict of interest statement
CONFLICT OF INTEREST DISCLOSURES
The authors made no disclosures.
Figures

References
-
- Layfield LJ, Wax TD, Lee JG, Cotton PB. Accuracy and morphologic aspects of pancreatic and biliary duct brushings. Acta Cytol. 1995;39:11–18. - PubMed
-
- Logrono R, Kurtycz D, Molina C, Trivedi V, Wong J, Block K. Analysis of false-negative diagnoses on endoscopic brush cytology of biliary and pancreatic duct strictures. Arch Pathol Lab Med. 2000;124:387–392. - PubMed
-
- Choi WT, Swanson PE, Grieco VS, Wang D, Westerhoff M. The outcomes of “atypical” and “suspicious” bile duct brushings in the identification of pancreaticobiliary tumors: follow-up analysis of surgical resection specimens. Diagn Cytopathol. 2015;43:885–891. - PubMed
-
- Okonkwo AM, De Frias DV, Gunn R, et al. Reclassification of “atypical” diagnoses in endoscopic retrograde cholangiopancreaticography–guided biliary brushings. Acta Cytol. 2003;47:435–442. - PubMed
-
- Volmar KE, Vollmer RT, Routbort MJ, Creager AJ. Pancreatic and bile duct brushing cytology in 1000 cases: review of findings and comparison of preparation methods. Cancer. 2006;108:231–238. - PubMed
