

Proximal small bowel obstruction in a patient with cystic fibrosis: a case report
- PMID: 31520190
- PMCID: PMC6744530
- DOI: 10.1186/s40792-019-0701-y
Proximal small bowel obstruction in a patient with cystic fibrosis: a case report
Abstract
Background: As advancements are made in the management of cystic fibrosis (CF), survival of the CF patient into adulthood has increased, leading to the discovery of previously unknown CF complications. Though gastrointestinal complications of CF, such as distal intestinal obstruction syndrome, are common, this case demonstrates a variant presentation of small bowel obstruction in this population.
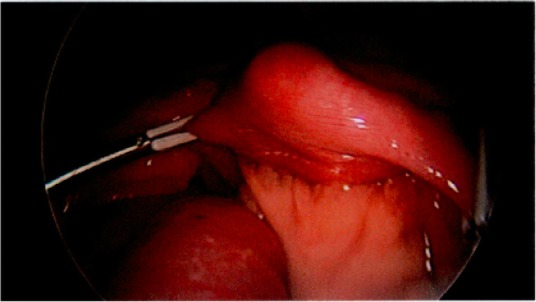
Case presentation: We describe a 42-year-old male with CF who presented with 2 days of worsening upper abdominal pain, emesis, and loss of bowel function. The patient had no history of any prior abdominal surgeries; however, imaging was concerning for high-grade mechanical small bowel obstruction possibly related to internal hernia. Given leukocytosis and diffusely tender abdomen found on further workup, the decision was made to proceed with diagnostic laparoscopy after a brief period of intravenous fluid resuscitation. Intraoperatively, the transition point was found in the mid-jejunum and was noted to be due to kinking of the bowel causing vascular congestion in the proximal portion. Surgical manipulation of the bowel was required for return of normal perfusion and patency.
Conclusion: Though the exact mechanism cannot be definitively delineated, we speculate that the increased viscosity and prolonged intestinal transit time, characteristic of CF, resulted in inspissated fecal content in the proximal small bowel, which then acted as a lead point for obstruction. Thus, though small bowel obstruction in patients with CF is often attributed to distal intestinal obstruction syndrome, a broader differential must be considered. Early surgical intervention may be necessary to prevent bowel ischemia and subsequent small bowel resection in a patient presenting with concerning clinical and image findings, as was seen in this patient.
Keywords: Abdominal pain; Cystic fibrosis; Distal intestinal obstruction syndrome; Small bowel obstruction; Surgical management.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures



References
-
- Smith VV, Schäppi MG, Bisset WM, Kiparissi F, Jaffe A, Milla PJ, et al. Lymphocytic leiomyositis and myenteric ganglionitis are intrinsic features of cystic fibrosis: studies in distal intestinal obstruction syndrome and meconium ileus. J Pediatr Gastroenterol Nutr. 2009;49(1):42–51. doi: 10.1097/MPG.0b013e318186d35a. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
