

Rhinovirus Type in Severe Bronchiolitis and the Development of Asthma
- PMID: 31520837
- PMCID: PMC7012669
- DOI: 10.1016/j.jaip.2019.08.043
Rhinovirus Type in Severe Bronchiolitis and the Development of Asthma
Abstract
Background: Respiratory syncytial virus (RSV)- and rhinovirus (RV)-induced bronchiolitis are associated with an increased risk of asthma, but more detailed information is needed on virus types.
Objective: To study whether RSV or RV types are differentially associated with the future use of asthma control medication.
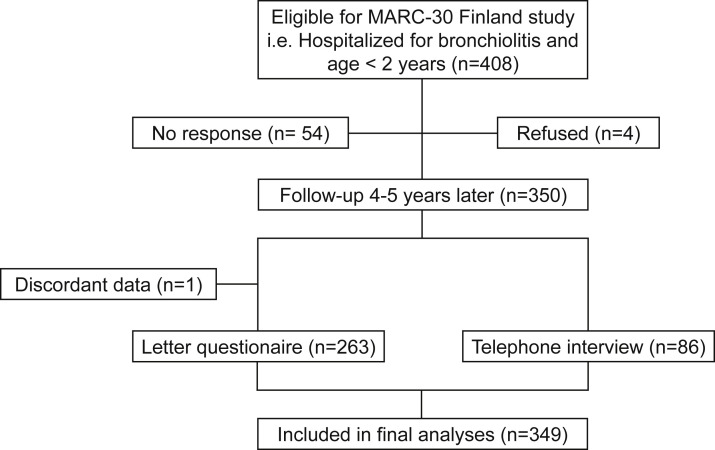
Methods: Over 2 consecutive winter seasons (2008-2010), we enrolled 408 children hospitalized for bronchiolitis at age less than 24 months into a prospective, 3-center, 4-year follow-up study in Finland. Virus detection was performed by real-time reverse transcription PCR from nasal wash samples. Four years later, we examined current use of asthma control medication.
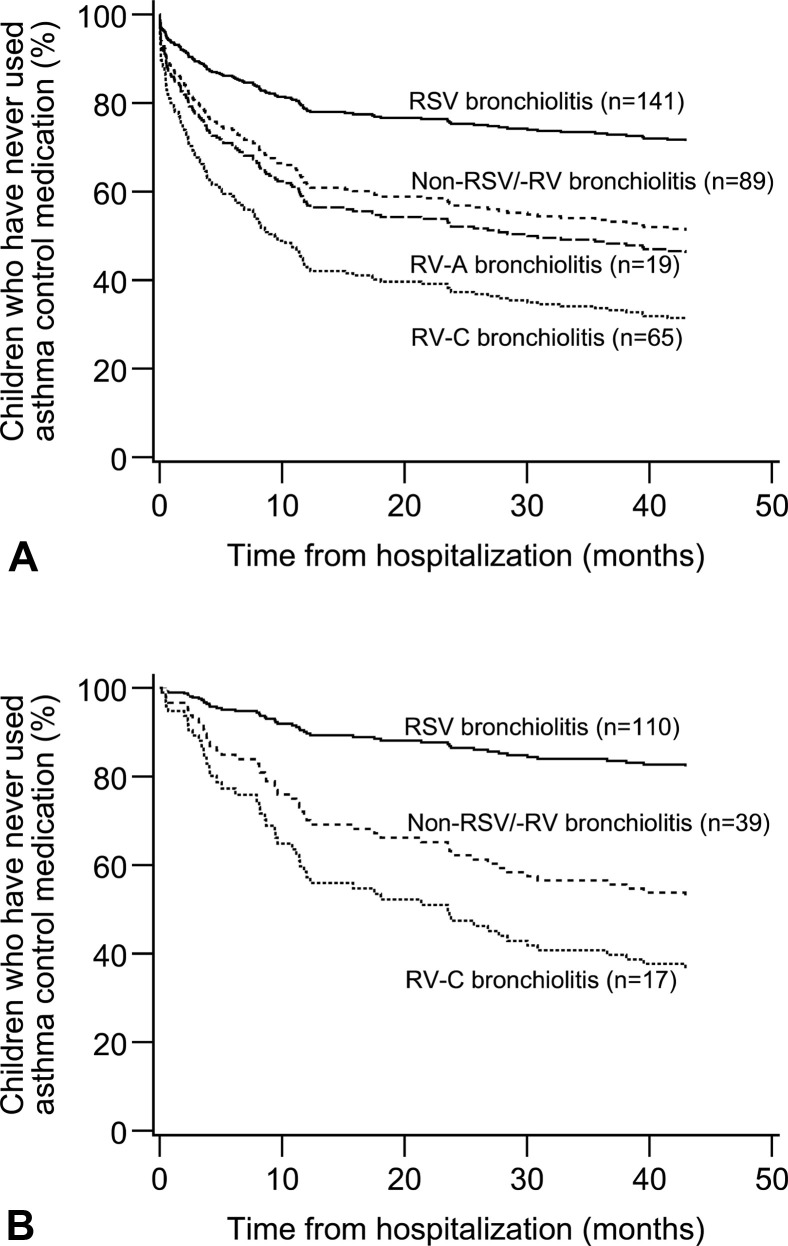
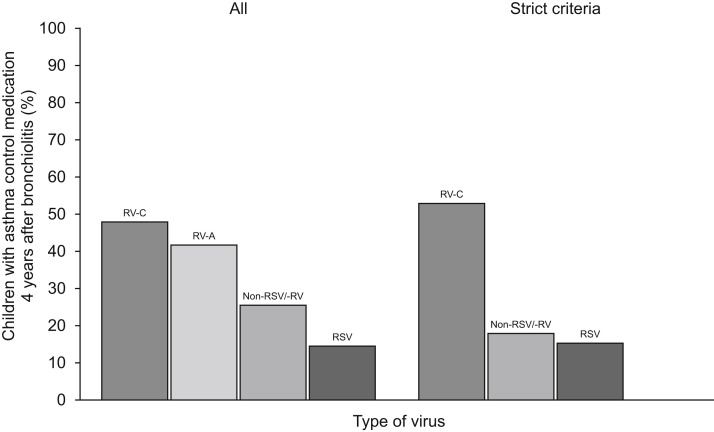
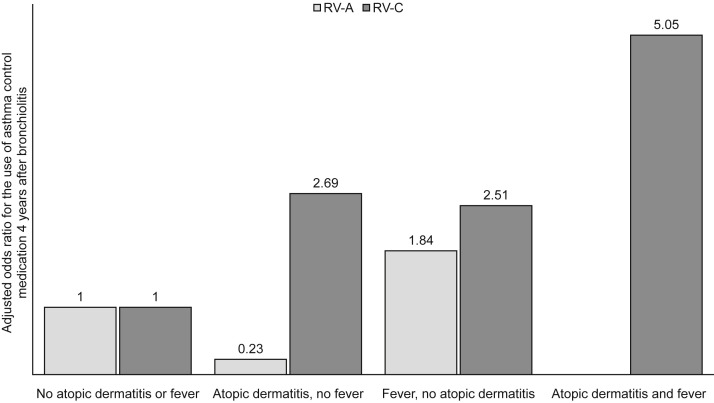
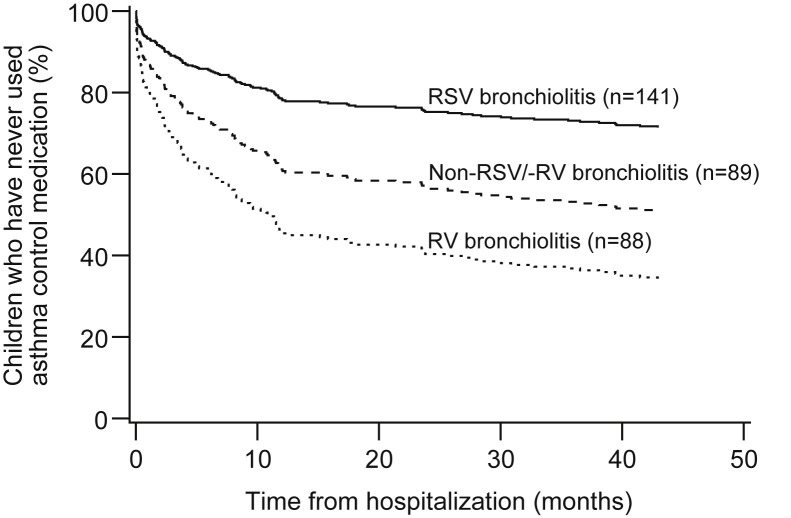
Results: A total of 349 (86%) children completed the 4-year follow-up. At study entry, the median age was 7.5 months, and 42% had RSV, 29% RV, 2% both RSV and RV, and 27% non-RSV/-RV etiology. The children with RV-A (adjusted hazard ratio, 2.3; P = .01), RV-C (adjusted hazard ratio, 3.5; P < .001), and non-RSV/-RV (adjusted hazard ratio, 2.0; P = .004) bronchiolitis started the asthma control medication earlier than did children with RSV bronchiolitis. Four years later, 27% of patients used asthma control medication; both RV-A (adjusted odds ratio, 3.0; P = .03) and RV-C (adjusted odds ratio, 3.7; P < .001) etiology were associated with the current use of asthma medication. The highest risk was found among patients with RV-C, atopic dermatitis, and fever (adjusted odds ratio, 5.0; P = .03).
Conclusions: Severe bronchiolitis caused by RV-A and RV-C was associated with earlier initiation and prolonged use of asthma control medication. The risk was especially high when bronchiolitis was associated with RV-C, atopic dermatitis, and fever.
Keywords: Asthma development; Bronchiolitis; Respiratory syncytial virus; Rhinovirus; Wheeze; Wheezing.
Copyright © 2019 American Academy of Allergy, Asthma & Immunology. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Ralston S.L., Lieberthal A.S., Meissner H.C., Alverson B.K., Baley J.E., Gadomski A.M. Clinical practice guideline: the diagnosis, management, and prevention of bronchiolitis. Pediatrics. 2014;134:e1474–e1502. - PubMed
-
- Meissner H.C. Viral bronchiolitis in children. N Engl J Med. 2016;374:62–72. - PubMed
-
- Balekian D.S., Linneman R.W., Hasegawa K., Ravi T., Camargo C.A. Cohort study of severe bronchiolitis during infancy and risk of asthma by age 5 years. J Allergy Clin Immunol Pract. 2017;5:92–96. - PubMed
