

Does Pentaerytrithyltetranitrate reduce fetal growth restriction in pregnancies complicated by uterine mal-perfusion? Study protocol of the PETN-study: a randomized controlled multicenter-trial
- PMID: 31521118
- PMCID: PMC6744635
- DOI: 10.1186/s12884-019-2456-7
Does Pentaerytrithyltetranitrate reduce fetal growth restriction in pregnancies complicated by uterine mal-perfusion? Study protocol of the PETN-study: a randomized controlled multicenter-trial
Abstract
Background: Affecting approximately 10% of pregnancies, fetal growth restriction (FGR), is the most important cause of perinatal mortality and morbidity. Impaired placental function and consequent mal-perfusion of the placenta is the leading cause of FGR. Although, screening for placental insufficiency based on uterine artery Doppler measurement is well established, there is no treatment option for pregnancies threatened by FGR. The organic nitrate pentaerithrityl tetranitrate (PETN) is widely used for the treatment of cardiovascular disease and has been shown to have protective effects on human endothelial cells. In a randomized placebo controlled pilot-study our group could demonstrate a risk reduction of 39% for the development of FGR, and FGR or death, by administering PETN to patients with impaired uterine artery Doppler at mid gestation. To confirm these results a prospective randomized placebo controlled double-blinded multicentre trial was now initiated.
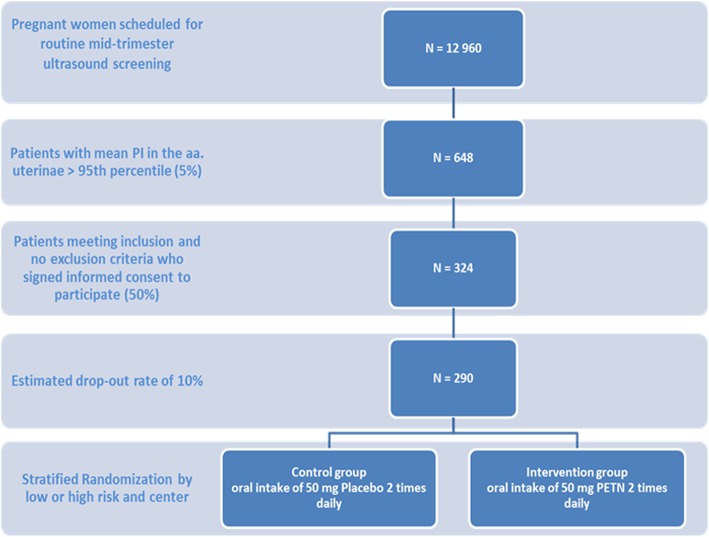
Method: The trial has been initiated in 14 centres in Germany. Inclusion criteria are abnormal uterine artery Doppler, defined by mean PI > 1.6, at 190 to 226 weeks of gestation in singleton pregnancies. Included patients will be monitored in 4-week intervals. Primary outcome measures are development of FGR (birth weight < 10th percentile), severe FGR (birth weight < 3rd centile) and perinatal death. Placental abruption, birth weight below the 3rd, 5th and 10th centile, development of FGR requiring delivery before 34 weeks` gestation, neonatal intensive care unit admission, and spontaneous preterm delivery < 34 weeks` and 37 weeks` gestation will be assessed as secondary endpoints. Patient enrolment was started in August 2017. Results are expected in 2020.
Discussion: During the past decade therapeutic agents with possible perfusion optimizing potential have been evaluated in clinical trials to treat FGR. Meta-analysis and sub-analysis of trials targeting preeclampsia revealed ASS to have a potential in reducing FGR. Phosphodiesterase-type-5 inhibitors have recently been tested in a worldwide RCT for therapy of established FGR, failing to show an effect on neonatal outcome. The ongoing multicenter trial will, by confirming our previous results, finally provide a therapeutic option in cases at risk for FGR.
Trial registration: DRKS00011374 registered at September 29th, 2017 and NCT03669185 , registered September 13th, 2018.
Keywords: Abnormal uterine Doppler; Fetal growth restriction; Nitric oxide (NO-) donors; Pentaerytrithyltetranitrate (PETN); Perinatal death.
Conflict of interest statement
The authors declare that they have no competing interests.
References
-
- Cnossen JS, Morris RK, ter Riet G, Mol BW, van der Post JA, Coomarasamy A, Zwinderman AH, Robson SC, Bindels PJ, Kleijnen J, et al. Use of uterine artery Doppler ultrasonography to predict pre-eclampsia and intrauterine growth restriction: a systematic review and bivariable meta-analysis. CMAJ. 2008;178(6):701–711. doi: 10.1503/cmaj.070430. - DOI - PMC - PubMed
-
- Yu CK, Smith GC, Papageorghiou AT, Cacho AM, Nicolaides KH. Fetal Medicine Foundation second trimester screening G: an integrated model for the prediction of preeclampsia using maternal factors and uterine artery Doppler velocimetry in unselected low-risk women. Am J Obstet Gynecol. 2005;193(2):429–436. doi: 10.1016/j.ajog.2004.12.014. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
