

Abbreviated quantitative UTE imaging in anterior cruciate ligament reconstruction
- PMID: 31521135
- PMCID: PMC6745079
- DOI: 10.1186/s12891-019-2811-x
Abbreviated quantitative UTE imaging in anterior cruciate ligament reconstruction
Abstract
Background: Existing ultrashort echo time magnetic resonance imaging (UTE MRI) methods require prohibitively long acquisition times (~ 20-40 min) to quantitatively assess the clinically relevant fast decay T2* component in ligaments and tendons. The purpose of this study was to evaluate the feasibility and clinical translatability of a novel abbreviated quantitative UTE MRI paradigm for monitoring graft remodeling after anterior cruciate ligament (ACL) reconstruction.
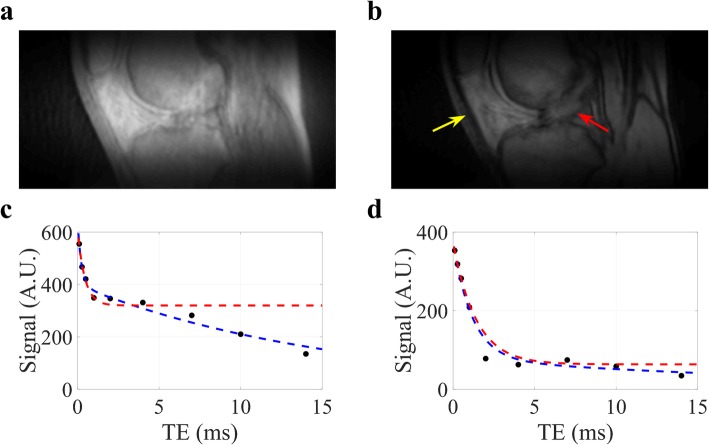
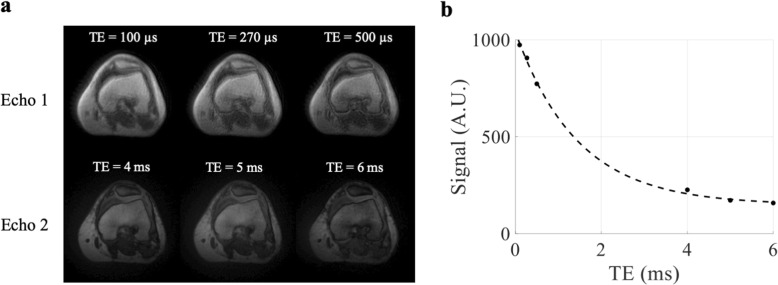
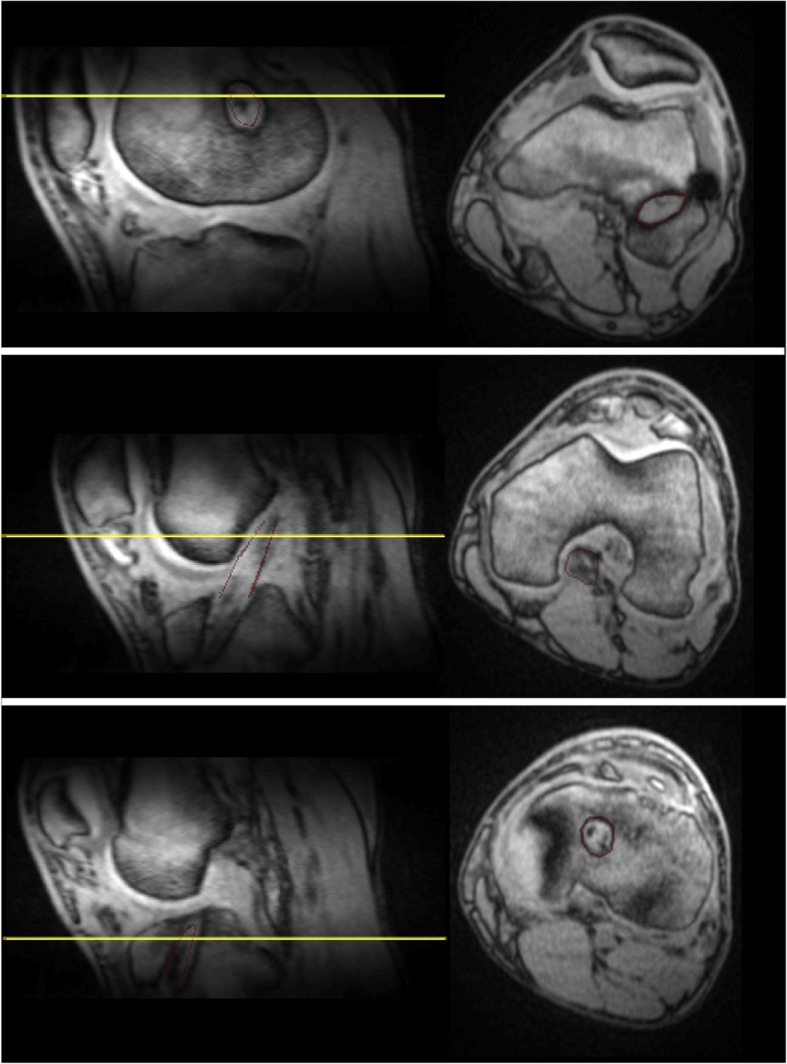
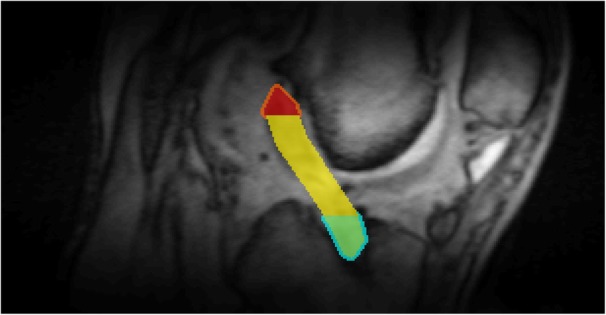
Methods: Eight patients who had Graftlink™ hamstring autograft reconstruction were recruited for this prospective study. A 3D double-echo UTE sequence at 3.0 Tesla was performed at 3- and 6-months post-surgery. An abbreviated UTE MRI paradigm was established based on numerical simulations and in vivo validation from healthy knees. This proposed approach was used to assess the T2* for fast decay component ([Formula: see text]) and bound water signal fraction (fbw) of ACL graft in regions of interest drawn by a radiologist.
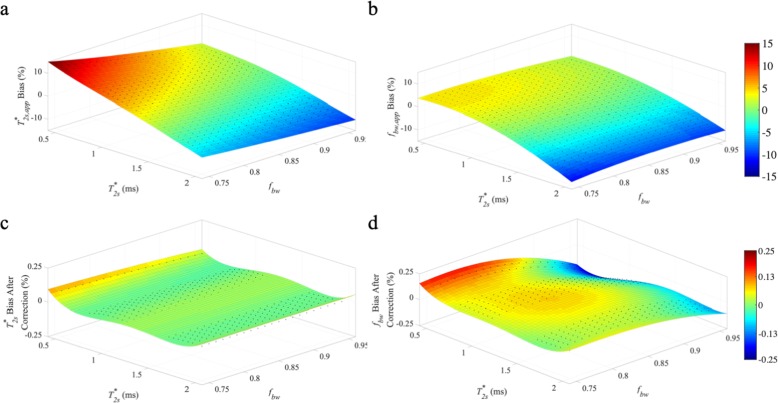
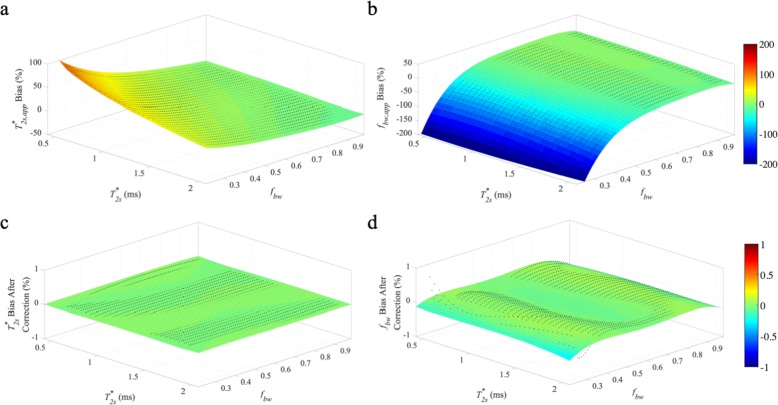
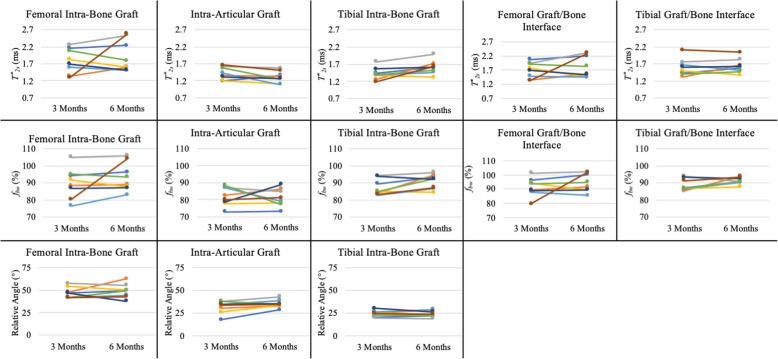
Results: Compared to the conventional bi-exponential model, the abbreviated UTE MRI paradigm achieved low relative estimation bias for [Formula: see text] and fbw over a range of clinically relevant values for ACL grafts. A decrease in [Formula: see text] of the intra-articular graft was observed in 7 of the 8 ACL reconstruction patients from 3- to 6-months (- 0.11 ± 0.16 ms, P = 0.10). Increases in [Formula: see text] and fbw from 3- to 6-months were observed in the tibial intra-bone graft ([Formula: see text]: 0.19 ± 0.18 ms, P < 0.05; Δfbw: 4% ± 4%, P < 0.05). Lower [Formula: see text] (- 0.09 ± 0.11 ms, P < 0.05) was observed at 3-months when comparing the intra-bone graft to the graft/bone interface in the femoral tunnel. The same comparisons at the 6-months also yielded relatively lower [Formula: see text] (- 0.09 ± 0.12 ms, P < 0.05).
Conclusion: The proposed abbreviated 3D UTE MRI paradigm is capable of assessing the ACL graft remodeling process in a clinically translatable acquisition time. Longitudinal changes in [Formula: see text] and fbw of the ACL graft were observed.
Keywords: ACL reconstruction; Anterior cruciate ligament (ACL); Graft healing; Ligamentization; Tendon-to-bone healing; Ultrashort TE (UTE).
Conflict of interest statement
Dr. James M. Paci is an educational consultant for and receives research support from Arthrex and Zimmer-Biomet.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
