

Hip-related groin pain, patient characteristics and patient-reported outcomes in patients referred to tertiary care due to longstanding hip and groin pain: a cross-sectional study
- PMID: 31521142
- PMCID: PMC6745069
- DOI: 10.1186/s12891-019-2794-7
Hip-related groin pain, patient characteristics and patient-reported outcomes in patients referred to tertiary care due to longstanding hip and groin pain: a cross-sectional study
Abstract
Background: Due to advances in hip arthroscopy, the number of surgical procedures has increased dramatically. The diagnostic challenge in patients with longstanding hip and groin pain, as well as the increasing number of hip arthroscopies, may lead to a higher number of patients referred to tertiary care for consideration for surgery. Therefore, the aims were: 1) to describe the prevalence of hip-related groin pain in patients referred to tertiary care due to longstanding hip and groin pain; and 2) to compare patient characteristics and patient-reported outcomes for patients categorized as having hip-related groin pain and those with non-hip-related groin pain.
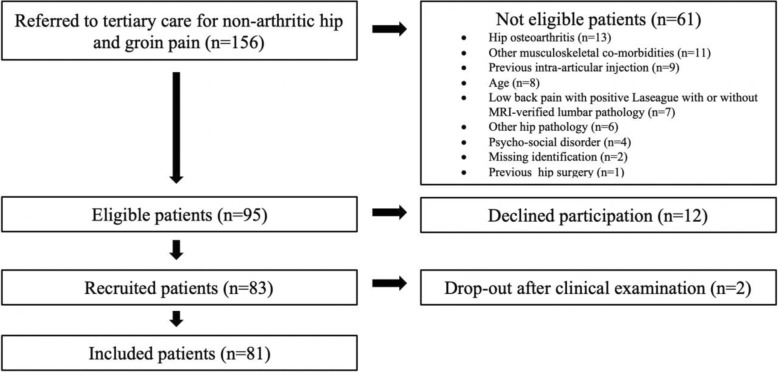
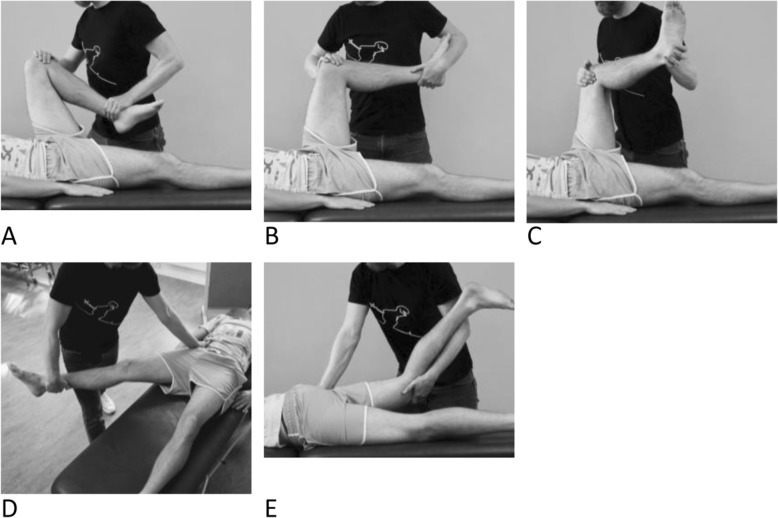
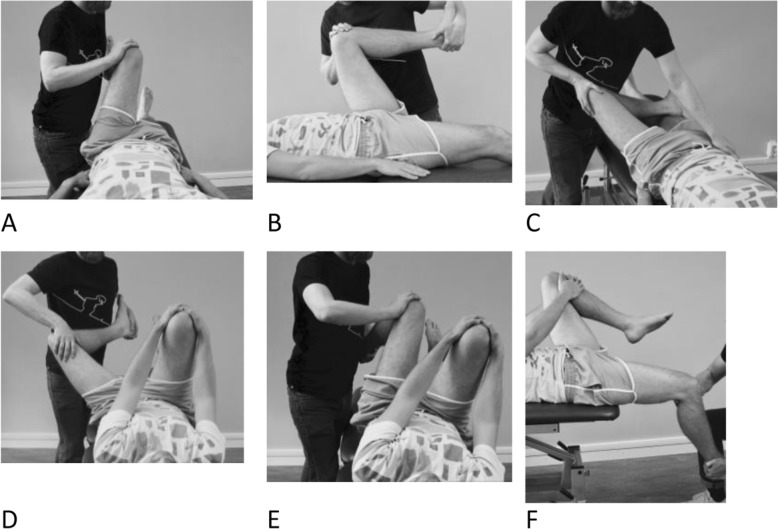
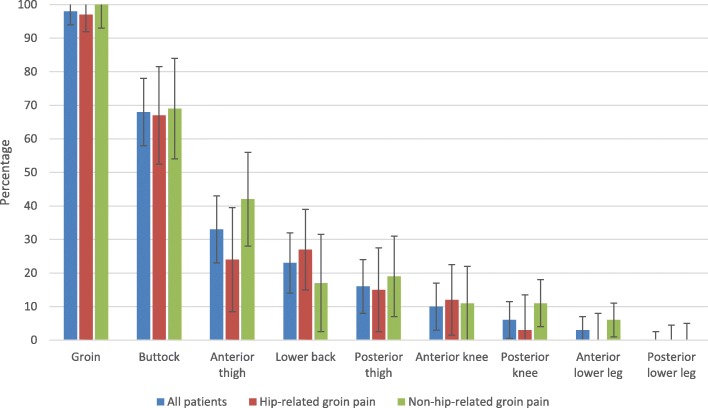
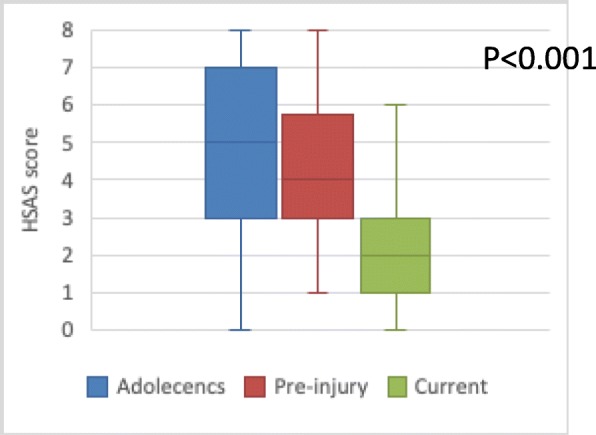
Methods: Eighty-one patients referred to the Department of Orthopedics at Skåne University Hospital for longstanding hip and groin pain were consecutively included and categorized into hip-related groin pain or non-hip-related groin pain using diagnostic criteria based on current best evidence (clinical examination, radiological examination and intra-articular block injection). Patient characteristics (gender (%), age (years), BMI (kg/m2)), results from the Hip Sports Activity Scale (HSAS), the SF-36, the Copenhagen Hip and Groin Outcome Score (HAGOS), and pain distribution (pain manikin) were collected. Parametric and non-parametric statistics were used as appropriate for between-group analysis.
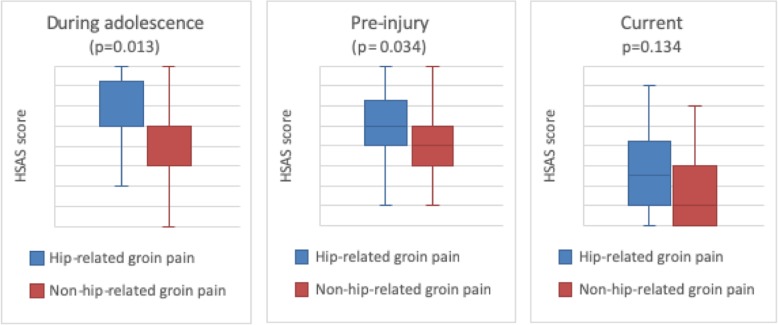
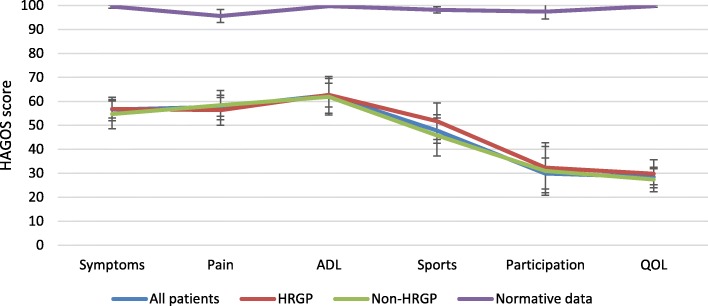
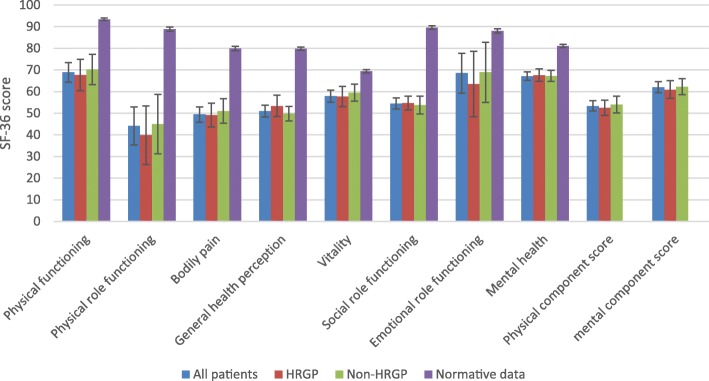
Results: Thirty-three (47%) patients, (30% women, 70% men, p < 0.01), were categorized as having hip-related groin pain. The hip-related groin pain group had a higher activity level during adolescence (p = 0.013), and a higher pre-injury activity level (p = 0.034), compared to the non-hip-related groin pain group. No differences (mean difference (95% CI)) between hip-related groin pain and non-hip-related groin pain were observed for age (0 (- 4; 4)), BMI (- 1.75 (- 3.61; 0.12)), any HAGOS subscales (p ≥ 0.318), any SF-36 subscales (p ≥ 0.142) or pain distribution (p ≥ 0.201).
Conclusions: Only half of the patients referred to tertiary care for long-standing hip and groin pain, who were predominantly men with a high activity level, had hip-related groin pain. Self-reported pain localization and distribution did not differ between patients with hip-related groin pain and those with non-hip-related groin pain, and both patient groups had poor perceived general health, and hip-related symptoms and function.
Keywords: Groin; Hip joint; Pain; Patient reported outcomes; Prevalence.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Patient-Reported Outcomes Within the First Year After Hip Arthroscopy and Rehabilitation for Femoroacetabular Impingement and/or Labral Injury: The Difference Between Getting Better and Getting Back to Normal.Am J Sports Med. 2018 Sep;46(11):2607-2614. doi: 10.1177/0363546518786971. Epub 2018 Aug 3. Am J Sports Med. 2018. PMID: 30074844 Clinical Trial.
-
Hip Joint Pathology as a Leading Cause of Groin Pain in the Sporting Population: A 6-Year Review of 894 Cases.Am J Sports Med. 2015 Jul;43(7):1698-703. doi: 10.1177/0363546515582031. Epub 2015 May 11. Am J Sports Med. 2015. PMID: 25964274
-
Danish Hip Arthroscopy Registry: predictors of outcome in patients with femoroacetabular impingement (FAI).Knee Surg Sports Traumatol Arthrosc. 2019 Oct;27(10):3110-3120. doi: 10.1007/s00167-018-4941-3. Epub 2018 Apr 25. Knee Surg Sports Traumatol Arthrosc. 2019. PMID: 29696319
-
[Femoroacetabular impingement of the hip in sports - a review for sports physicians].Sportverletz Sportschaden. 2010 Sep;24(3):133-9. doi: 10.1055/s-0029-1245408. Epub 2010 Sep 15. Sportverletz Sportschaden. 2010. PMID: 20845240 Review. German.
-
Femoroacetabular impingement: a common cause of hip pain.Phys Sportsmed. 2018 May;46(2):139-144. doi: 10.1080/00913847.2018.1436844. Epub 2018 Feb 13. Phys Sportsmed. 2018. PMID: 29406812 Review.
Cited by
-
Less hip range of motion is associated with a greater alpha angle in people with longstanding hip and groin pain.Knee Surg Sports Traumatol Arthrosc. 2021 Dec;29(12):4091-4099. doi: 10.1007/s00167-021-06733-2. Epub 2021 Sep 12. Knee Surg Sports Traumatol Arthrosc. 2021. PMID: 34510222 Free PMC article.
-
Sex Differences in Patient-Reported Outcomes Following Surgical Hip Preservation Interventions: A Systematic Review and Meta-Analysis.Iowa Orthop J. 2023 Dec;43(2):133-145. Iowa Orthop J. 2023. PMID: 38213859 Free PMC article.
-
Clinical assessment and treatment of patients presenting with longstanding hip and groin pain in primary care: a survey study among physical therapists and general practitioners in Sweden.BMC Musculoskelet Disord. 2025 Mar 3;26(1):218. doi: 10.1186/s12891-025-08466-6. BMC Musculoskelet Disord. 2025. PMID: 40033287 Free PMC article.
-
Google Trends for Pain Search Terms in the World's Most Populated Regions Before and After the First Recorded COVID-19 Case: Infodemiological Study.J Med Internet Res. 2021 Apr 22;23(4):e27214. doi: 10.2196/27214. J Med Internet Res. 2021. PMID: 33844638 Free PMC article.
-
Soccer players show the highest seasonal groin pain prevalence and the longest time loss from sport among 500 athletes from major team sports.Knee Surg Sports Traumatol Arthrosc. 2022 Jun;30(6):2149-2157. doi: 10.1007/s00167-022-06924-5. Epub 2022 Mar 8. Knee Surg Sports Traumatol Arthrosc. 2022. PMID: 35258646
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
