

Meta-analysis of Temporal and Surgical Risk Dependent Associations With Outcomes After Transcatheter Versus Surgical Aortic Valve Implantation
- PMID: 31521258
- PMCID: PMC7453964
- DOI: 10.1016/j.amjcard.2019.07.066
Meta-analysis of Temporal and Surgical Risk Dependent Associations With Outcomes After Transcatheter Versus Surgical Aortic Valve Implantation
Abstract
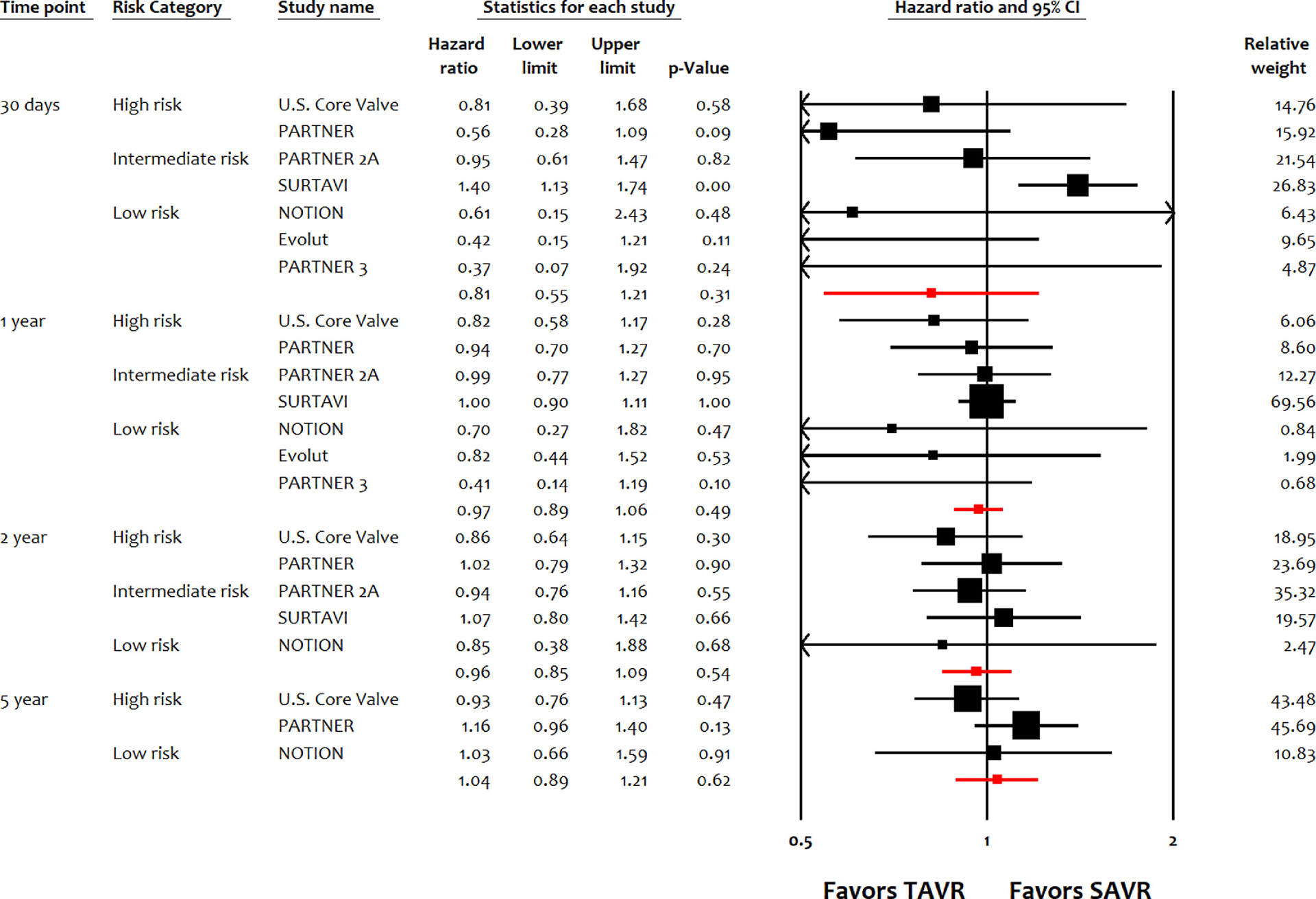
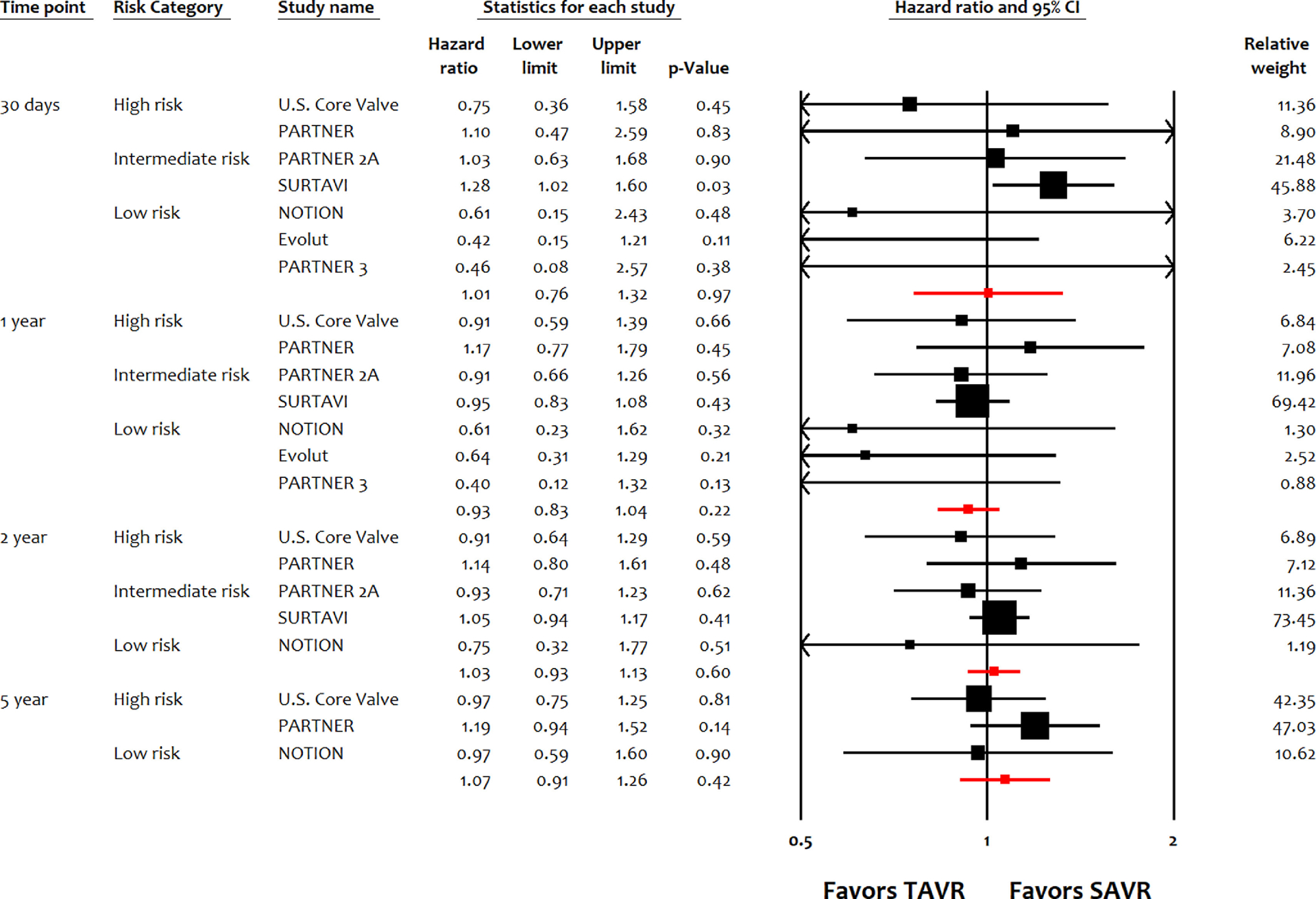
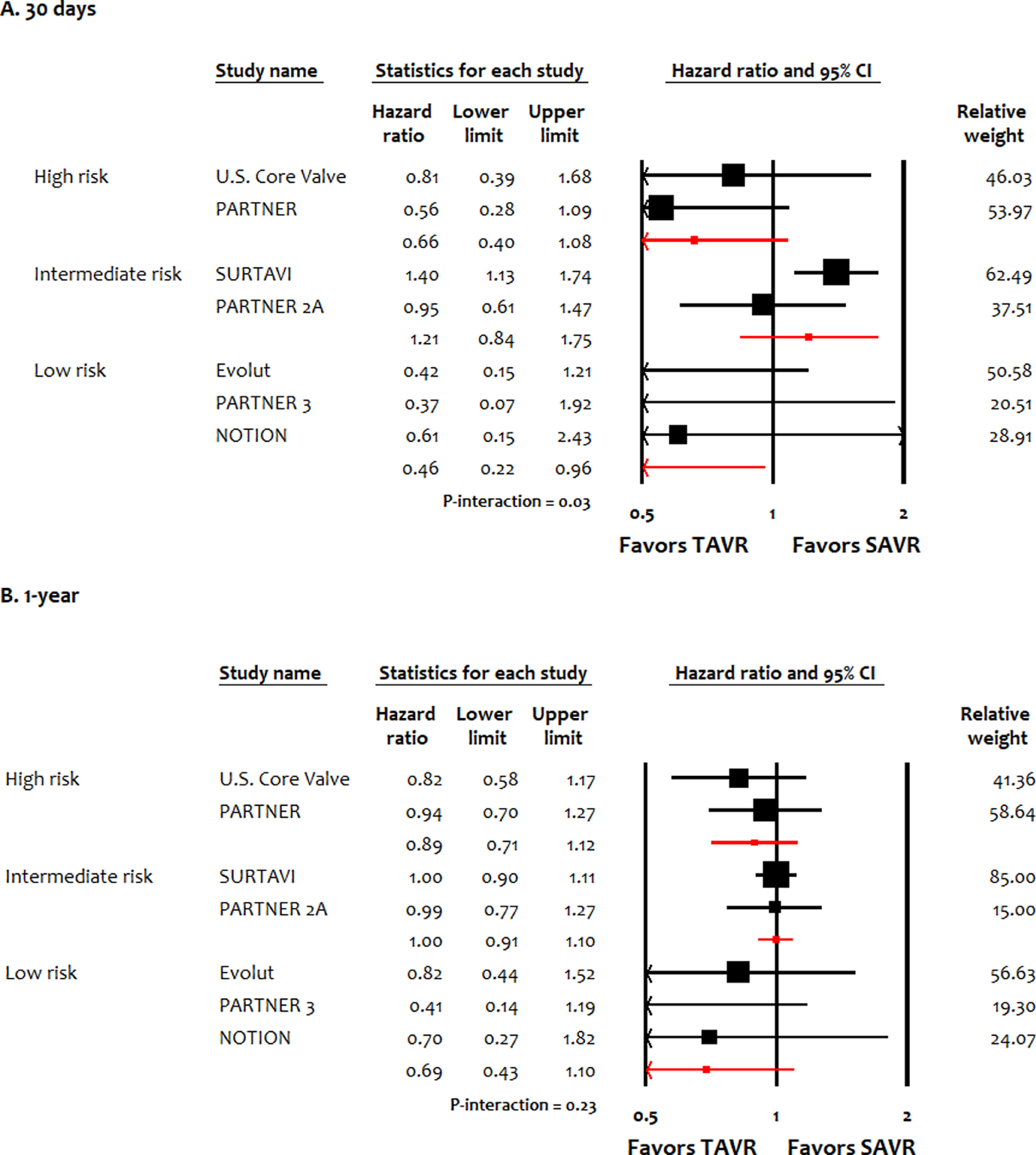
Temporal and surgical risk dependent associations with clinical outcomes in patients receiving transcatheter versus surgical aortic valve implantation (TAVI vs SAVI) are uncertain. In this meta-analysis, 7 randomized controlled trials (7,771 patients) were included to investigate trends in outcomes in TAVI versus SAVI up to 5 years, and variation in outcomes with respect to low-, intermediate-, and high-surgical risk of the patients up to 1 year. Estimates were calculated as random effects hazard ratios (HRs) with 95% confidence intervals (CI). All-cause mortality was similar in TAVI and SAVI at 30 days (HR 0.81, 95% CI 0.55 to 1.21, p = 0.31), 1 year (HR 0.97, 95% CI 0.89 to 1.06, p = 0.49), 2 years (HR 0.96, 95 CI 0.85 to 1.09, p = 0.54), and 5 years (HR 1.04, 95% CI 0.89 to 1.21, p = 0.62). Cardiac mortality, myocardial infarction and stroke were similar in both interventions up to 5 years. TAVI was associated with lower risk of atrial fibrillation, but higher risk of vascular complications, pacemaker implantation, and paravalvular leak up to 5 years. The lower risks of major bleeding and acute kidney injury with TAVI versus SAVI were limited to 1 and 2 years, respectively. Compared with SAVI, TAVI was superior in reducing all-cause mortality in low surgical risk patients at 30 days only, whereas TAVI was noninferior to SAVI in intermediate- and high-risk patients at 30 days and across all risks at 1 year. In conclusion, TAVI was noninferior to SAVI in terms of mortality, myocardial infarction, and stroke up to 5 years. TAVI improved survival versus SAVI in low-risk patients at 30 days.
Copyright © 2019 Elsevier Inc. All rights reserved.
Conflict of interest statement
Disclosures
The authors have no conflicts of interest to disclose.
Figures
References
-
- Nishimura RA, Otto CM, Bonow RO, Carabello BA, Erwin JP 3rd, Fleisher LA, Jneid H, Mack MJ, McLeod CJ, O’Gara PT, Rigolin VH, Sundt TM 3rd, Thompson A. 2017 AHA/ACC focused update of the 2014 AHA/ACC guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2017;135:e1159–e1195. - PubMed
-
- Gargiulo G, Sannino A, Capodanno D, Barbanti M, Buccheri S, Perrino C, Capranzano P, Indolfi C, Trimarco B, Tamburino C, Esposito G. Transcatheter aortic valve implantation versus surgical aortic valve replacement: a systematic review and Meta-analysis. Ann Intern Med 2016;165:334–344. - PubMed
-
- Popma JJ, Deeb GM, Yakubov SJ, Mumtaz M, Gada H, O’Hair D, Bajwa T, Heiser JC, Merhi W, Kleiman NS, Askew J, Sorajja P, Rovin J, Chetcuti SJ, Adams DH, Teirstein PS, Zorn GL 3rd, Forrest JK, Tch etch e D, Resar J, Walton A, Piazza N, Ramlawi B, Robinson N, Petrossian G, Gleason TG, Oh JK, Boulware MJ, Qiao H, Mugglin AS, Reardon MJ. Transcatheter aortic-valve replacement with a self-expanding valve in low-risk patients. N Engl J Med 2019;380:1706–1715. - PubMed
-
- Mack MJ, Leon MB, Thourani VH, Makkar R, Kodali SK, Russo M, Kapadia SR, Malaisrie SC, Cohen DJ, Pibarot P, Leipsic J, Hahn RT, Blanke P, Williams MR, McCabe JM, Brown DL, Babaliaros V, Goldman S, Szeto WY, Genereux P, Pershad A, Pocock SJ, Alu MC, Webb JG, Smith CR. Transcatheter aortic-valve replacement with a balloon-expandable valve in low-risk patients. N Engl J Med 2019;380:1695–1705. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
