

Progress in cancer survival, mortality, and incidence in seven high-income countries 1995-2014 (ICBP SURVMARK-2): a population-based study
- PMID: 31521509
- PMCID: PMC6838671
- DOI: 10.1016/S1470-2045(19)30456-5
Progress in cancer survival, mortality, and incidence in seven high-income countries 1995-2014 (ICBP SURVMARK-2): a population-based study
Abstract
Background: Population-based cancer survival estimates provide valuable insights into the effectiveness of cancer services and can reflect the prospects of cure. As part of the second phase of the International Cancer Benchmarking Partnership (ICBP), the Cancer Survival in High-Income Countries (SURVMARK-2) project aims to provide a comprehensive overview of cancer survival across seven high-income countries and a comparative assessment of corresponding incidence and mortality trends.
Methods: In this longitudinal, population-based study, we collected patient-level data on 3·9 million patients with cancer from population-based cancer registries in 21 jurisdictions in seven countries (Australia, Canada, Denmark, Ireland, New Zealand, Norway, and the UK) for seven sites of cancer (oesophagus, stomach, colon, rectum, pancreas, lung, and ovary) diagnosed between 1995 and 2014, and followed up until Dec 31, 2015. We calculated age-standardised net survival at 1 year and 5 years after diagnosis by site, age group, and period of diagnosis. We mapped changes in incidence and mortality to changes in survival to assess progress in cancer control.
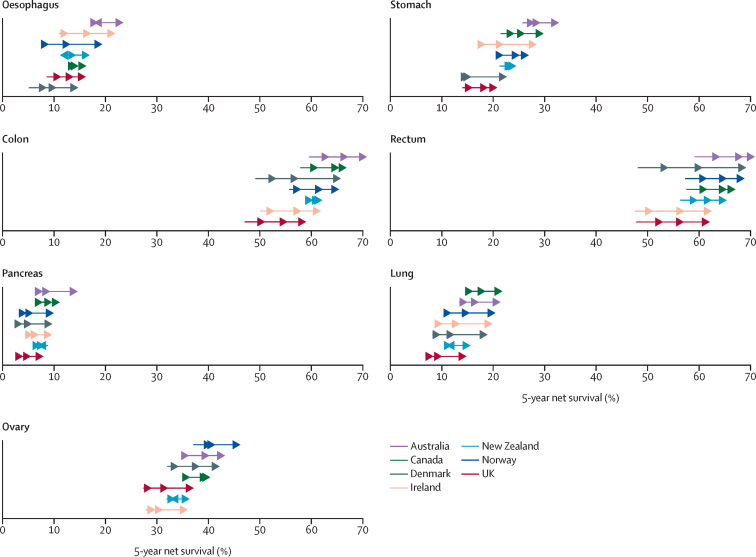
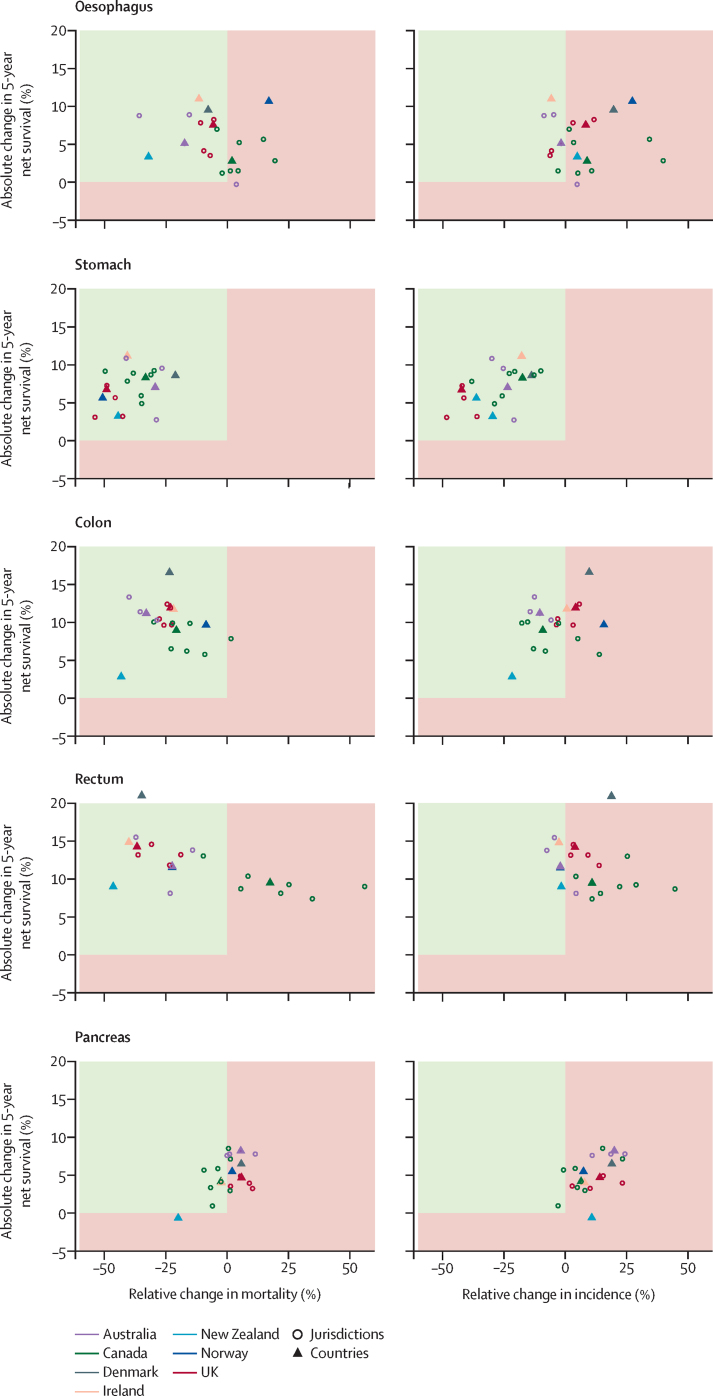
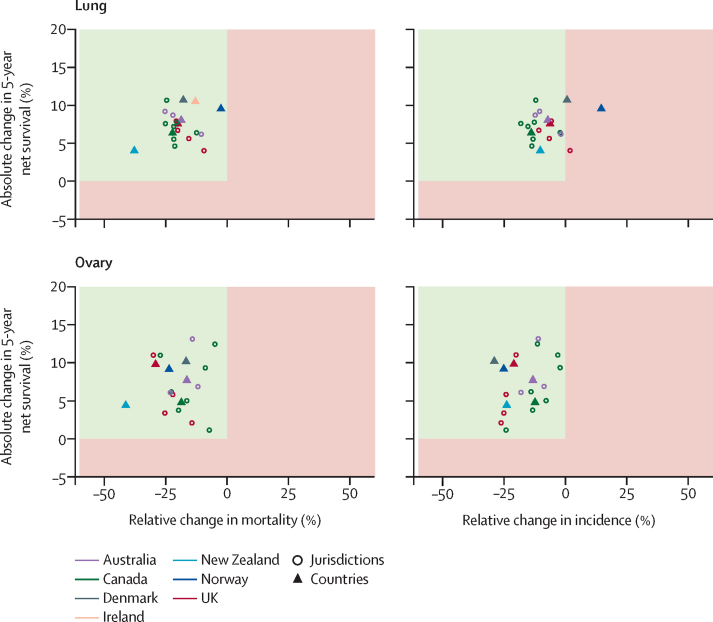
Findings: In 19 eligible jurisdictions, 3 764 543 cases of cancer were eligible for inclusion in the study. In the 19 included jurisdictions, over 1995-2014, 1-year and 5-year net survival increased in each country across almost all cancer types, with, for example, 5-year rectal cancer survival increasing more than 13 percentage points in Denmark, Ireland, and the UK. For 2010-14, survival was generally higher in Australia, Canada, and Norway than in New Zealand, Denmark, Ireland, and the UK. Over the study period, larger survival improvements were observed for patients younger than 75 years at diagnosis than those aged 75 years and older, and notably for cancers with a poor prognosis (ie, oesophagus, stomach, pancreas, and lung). Progress in cancer control (ie, increased survival, decreased mortality and incidence) over the study period was evident for stomach, colon, lung (in males), and ovarian cancer.
Interpretation: The joint evaluation of trends in incidence, mortality, and survival indicated progress in four of the seven studied cancers. Cancer survival continues to increase across high-income countries; however, international disparities persist. While truly valid comparisons require differences in registration practice, classification, and coding to be minimal, stage of disease at diagnosis, timely access to effective treatment, and the extent of comorbidity are likely the main determinants of patient outcomes. Future studies are needed to assess the impact of these factors to further our understanding of international disparities in cancer survival.
Funding: Canadian Partnership Against Cancer; Cancer Council Victoria; Cancer Institute New South Wales; Cancer Research UK; Danish Cancer Society; National Cancer Registry Ireland; The Cancer Society of New Zealand; National Health Service England; Norwegian Cancer Society; Public Health Agency Northern Ireland, on behalf of the Northern Ireland Cancer Registry; The Scottish Government; Western Australia Department of Health; and Wales Cancer Network.
© This is an Open Access article published under the CC BY-NC-ND 3.0 IGO license which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. In any use of this article, there should be no suggestion that WHO endorses any specific organisation, products or services. The use of the WHO logo is not permitted. This notice should be preserved along with the article's original URL.
Figures
Comment in
-
UK's poor performance on cancer survival.BMJ. 2019 Oct 28;367:l6122. doi: 10.1136/bmj.l6122. BMJ. 2019. PMID: 31658950 No abstract available.
-
Are health-care policies restricting further progress in cancer survival outcomes?Lancet Oncol. 2019 Dec;20(12):e657. doi: 10.1016/S1470-2045(19)30749-1. Lancet Oncol. 2019. PMID: 31797783 No abstract available.
References
-
- Butler J, Foot C, Bomb M. The International Cancer Benchmarking Partnership: an international collaboration to inform cancer policy in Australia, Canada, Denmark, Norway, Sweden and the United Kingdom. Health Policy. 2013;112:148–155. - PubMed
-
- SURVMARK: cancer survival in high-income countries. International Agency for Research on Cancer, World Health Oragniaztion. http://survival.iarc.fr/Survmark/en/
-
- De Angelis R, Sant M, Coleman MP. Cancer survival in Europe 1999–2007 by country and age: results of EUROCARE-5— a population-based study. Lancet Oncol. 2014;15:23–34. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
