

CABG Improves Outcomes in Patients With Ischemic Cardiomyopathy: 10-Year Follow-Up of the STICH Trial
- PMID: 31521682
- PMCID: PMC7375257
- DOI: 10.1016/j.jchf.2019.04.018
CABG Improves Outcomes in Patients With Ischemic Cardiomyopathy: 10-Year Follow-Up of the STICH Trial
Abstract
Objectives: The authors investigated the impact of coronary artery bypass grafting (CABG) on first and recurrent hospitalization in this population.
Background: In the STICH (Surgical Treatment for Ischemic Heart Failure) trial, CABG reduced all-cause death and hospitalization in patients with and ischemic cardiomyopathy and left ventricular ejection fraction <35%.
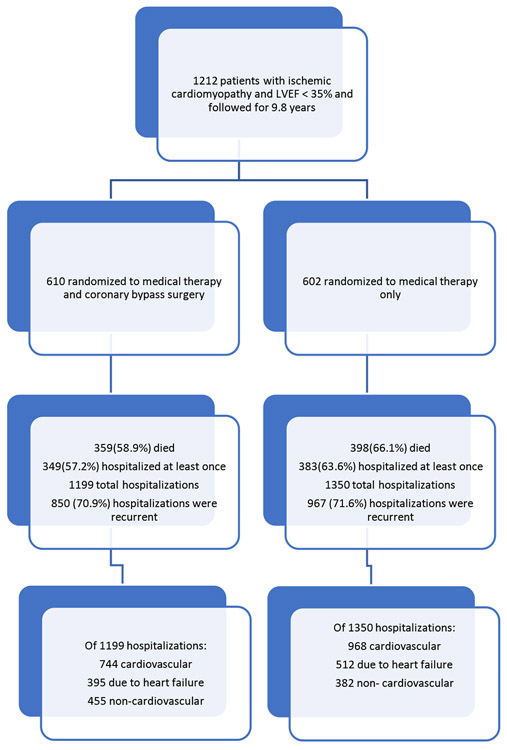
Methods: A total of 1,212 patients were randomized (610 to CABG + optimal medical therapy [CABG] and 602 to optimal medical therapy alone [MED] alone) and followed for a median of 9.8 years. All-cause and cause-specific hospitalizations were analyzed as time-to-first-event and as recurrent event analysis.
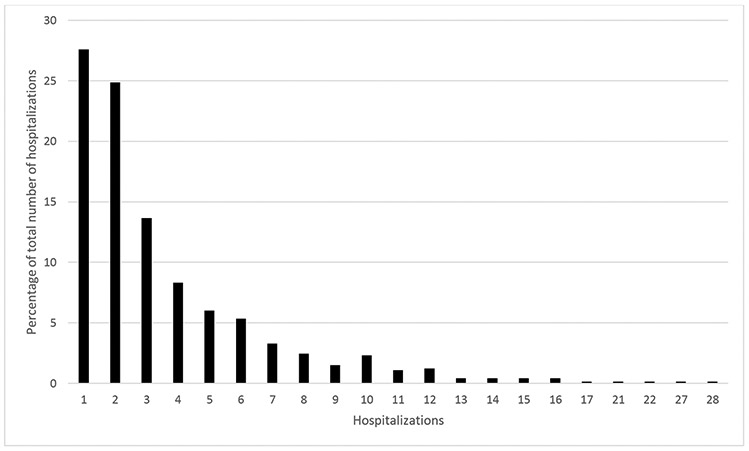
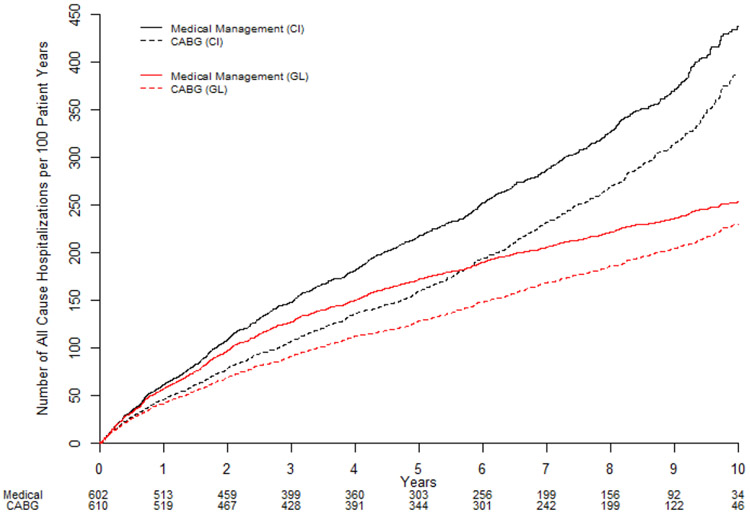
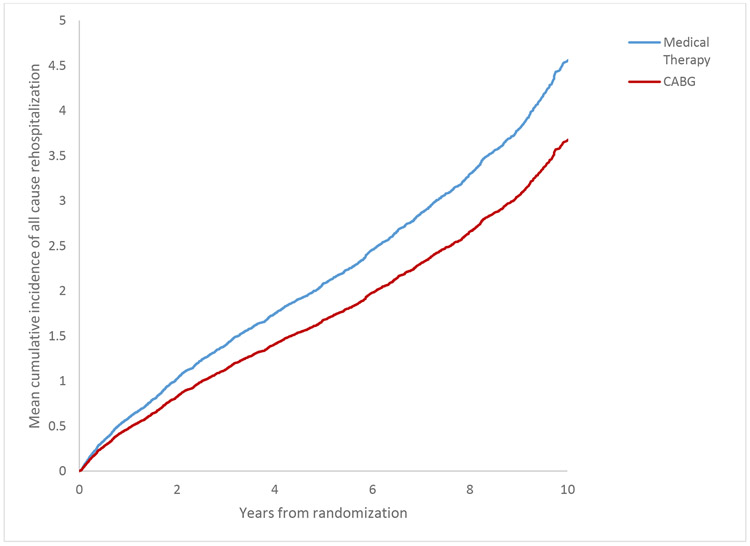
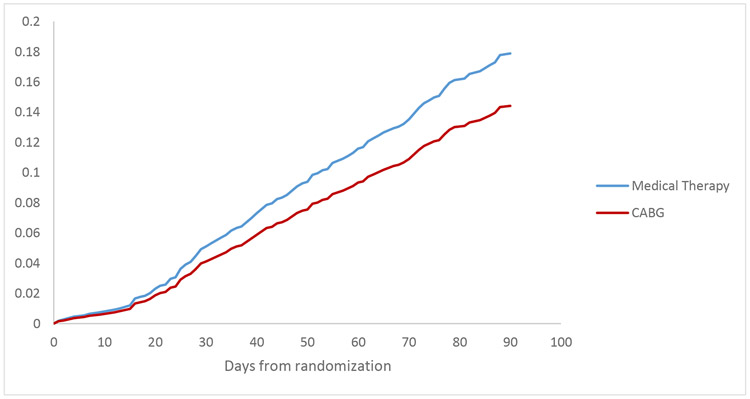
Results: Of the 1,212 patients, 757 died (62.4%) and 732 (60.4%) were hospitalized at least once, for a total of 2,549 total all-cause hospitalizations. Most hospitalizations (66.2%) were for cardiovascular causes, of which approximately one-half (907 or 52.9%) were for heart failure. More than 70% of all hospitalizations (1,817 or 71.3%) were recurrent events. The CABG group experienced fewer all-cause hospitalizations in the time-to-first-event (349 CABG vs. 383 MED, adjusted hazard ratio [HR]: 0.85; 95% confidence interval [CI]: 0.74 to 0.98; p = 0.03) and in recurrent event analyses (1,199 CABG vs. 1,350 MED, HR: 0.78, 95% CI: 0.65 to 0.94; p < 0.001). This was driven by fewer total cardiovascular (CV) hospitalizations (744 vs. 968; p < 0.001, adjusted HR: 0.66, 95% CI: 0.55 to 0.81; p = 0.001), the majority of which were due to HF (395 vs. 512; p < 0.001, adjusted HR: 0.68, 95% CI: 0.52-0.89; p = 0.005). We did not observe a difference in non-CV events.
Conclusions: CABG reduces all-cause, CV, and HF hospitalizations in time-to-first-event and recurrent event analyses. (Comparison of Surgical and Medical Treatment for Congestive Heart Failure and Coronary Artery Disease [STICH]; NCT00023595).
Keywords: coronary artery bypass grafting; heart failure; hospitalization; ischemic cardiomyopathy; morbidity.
Copyright © 2019 American College of Cardiology Foundation. All rights reserved.
Figures
Comment in
-
The Risk of Dying From and the Prospect of Living With Ischemic Cardiomyopathy.JACC Heart Fail. 2019 Oct;7(10):888-890. doi: 10.1016/j.jchf.2019.05.007. Epub 2019 Sep 11. JACC Heart Fail. 2019. PMID: 31521685 No abstract available.
References
-
- Shen L, Jhund PS, Mogensen UM et al. Re-Examination of the BEST Trial Using Composite Outcomes, Including Emergency Department Visits. JACC Heart Fail 2017;5:591–599. - PubMed
-
- Skali H, Pfeffer MA, Lubsen J, Solomon SD. Variable impact of combining fatal and nonfatal end points in heart failure trials. Circulation 2006;114:2298–303. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
