

Phase II randomised discontinuation trial of brivanib in patients with advanced solid tumours
- PMID: 31522033
- PMCID: PMC8852771
- DOI: 10.1016/j.ejca.2019.07.024
Phase II randomised discontinuation trial of brivanib in patients with advanced solid tumours
Abstract
Background: Brivanib is a selective inhibitor of vascular endothelial growth factor and fibroblast growth factor (FGF) signalling. We performed a phase II randomised discontinuation trial of brivanib in 7 tumour types (soft-tissue sarcomas [STS], ovarian cancer, breast cancer, pancreatic cancer, non-small-cell lung cancer [NSCLC], gastric/esophageal cancer and transitional cell carcinoma [TCC]).
Patients and methods: During a 12-week open-label lead-in period, patients received brivanib 800 mg daily and were evaluated for FGF2 status by immunohistochemistry. Patients with stable disease at week 12 were randomised to brivanib or placebo. A study steering committee evaluated week 12 response to determine if enrolment in a tumour type would continue. The primary objective was progression-free survival (PFS) for brivanib versus placebo in patients with FGF2-positive tumours.
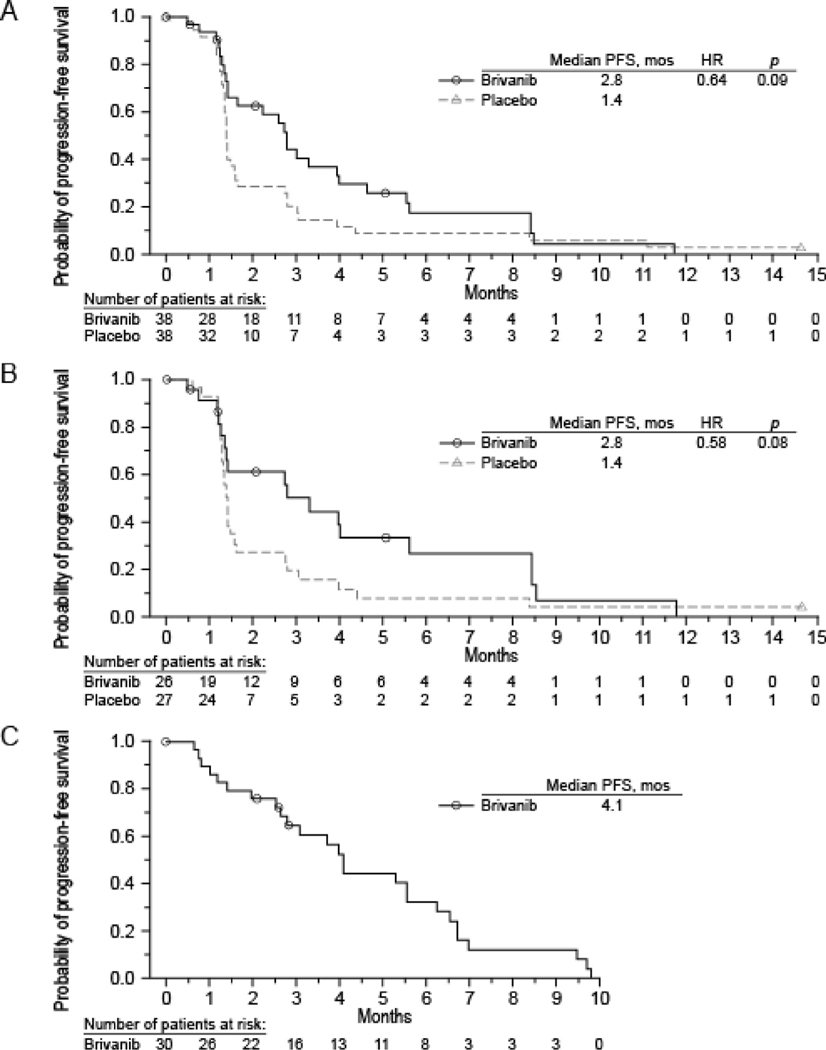
Results: A total of 595 patients were treated, and stable disease was observed at the week 12 randomisation point in all tumour types. Closure decisions were made for breast cancer, pancreatic cancer, NSCLC, gastric cancer and TCC. Criteria for expansion were met for STS and ovarian cancer. In 53 randomised patients with STS and FGF2-positive tumours, the median PFS was 2.8 months for brivanib and 1.4 months for placebo (hazard ratio [HR]: 0.58, p = 0.08). For all randomised patients with sarcomas, the median PFS was 2.8 months (95% confidence interval [CI]: 1.4-4.0) for those treated with brivanib compared with 1.4 months (95% CI: 1.3-1.6) for placebo (HR = 0.64, 95% CI: 0.38-1.07; p = 0.09). In the 36 randomised patients with ovarian cancer and FGF2-positive tumours, the median PFS was 4.0 (95% CI: 2.6-4.2) months for brivanib and 2.0 months (95% CI: 1.2-2.7) for placebo (HR: 0.56, 95% CI: 0.26-1.22). For all randomised patients with ovarian cancer, the median PFS in those randomised to brivanib was 4.0 months (95% CI: 2.6-4.2) and was 2.0 months (95% CI: 1.2-2.7) in those randomised to placebo (HR = 0.54, 95% CI: 0.25-1.17; p = 0.11).
Conclusion: Brivanib demonstrated activity in STS and ovarian cancer with an acceptable safety profile. FGF2 expression, as defined in the protocol, is not a predictive biomarker of the efficacy of brivanib.
Keywords: Brivanib; FGF2 status; Ovarian cancer; Randomised discontinuation trial; Sarcomas; Solid tumours.
Copyright © 2019 The Author(s). Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Conflict of interest statement
Robin L Jones has been a consultant for Adaptimmune, Blueprint, Clinigen, Eisai, Epizyme, Daichii, Deciphera, Immunedesign, Lilly, Merck, Pharmamar, Tracon, Upto Date.
Mark Ratain reports receiving grants from AbbVie, Dicerna and Genentech, reports receiving personal fees from AbbVie, Amgen, Ascentage, Cyclacel, Elion Oncology, multiple generic pharmaceutical companies, Shionogi and Portola Pharmaceuticals, outside the submitted work, is a coinventor on patent US6395481B1 with royalties paid from Mayo Clinic, patent US20160239636A1 pending, patent US8877723B2 issued and patent EP1629111B1 with royalties paid from Mayo Clinic, and serves as a director and treasurer of the Value in Cancer Care Consortium.
Peter J. O’Dwyer reports research support from Pfizer, Genentech, BMS, GSK, Five Prime, Forty Seven, BBI, Novartis, Celgene, Incyte, Lilly / Imclone, Array, H3 Biomedicine and Taiho Pharma, has been consulting in the past 2 years for Genentech, Celgene and Array, provides expert testimony for Bayer and Lilly and is not a stock owner of any companies.
Lillian Siu serves as a consultant for Merck (compensated), Pfizer (compensated), Celgene (compensated), AstraZeneca/MedImmune (compensated), MorphoSys (compensated), Roche (compensated), Geneseeq (compensated), Loxo (compensated), Oncorus (compensated), Symphogen (compensated), Seattle Genetics (compensated) and GSK (compensated), is not a member of the speaker’s bureau for any companies, reports grant/research support (clinical trials for institution) from Novartis, Bristol-Myers Squibb, Pfizer, Boehringer-Ingelheim, GlaxoSmithKline, Roche/Genentech, Karyopharm Therapeutics, Inc., AstraZeneca/MedImmune, Merck, Celgene, Astellas, Bayer, AbbVie, Amgen, Symphogen, Intensity Therapeutics, Mirati and Shattucksm Avid, is a stockholder of Agios (spouse) and is not an employee of any companies.
Jacek Jassem serves as a speaker for AstraZeneca, Roche and Pfizer and reports advisory roles for AstraZeneca, BMS, Pfizer, MSD and Takeda and travel support from Roche.
Jacques Medioni reports honoraria and advisory roles from Pierre Fabre, AstraZeneca, Invectys and Astellas.
Robert Maki reports consulting fees from Arcus, Bayer, Deciphera, Eisai, Immune Design, Janssen R&D, Karyopharm Therapeutics, Lilly, Novartis, Pfizer, Presage, Sarcoma Alliance for Research Through Collaboration (SARC), SpringWorks, American Board of Internal Medicine and UpToDate and reports institutional receipts for clinical trials from Bayer, Karyopharm, Lilly, Pfizer, Regeneron, Presage, Sarcoma Alliance for Research Through Collaboration (SARC), SpringWorks and Tracon.
Ian Walters is an employee/stock owner of BMS at the time of the study and is currently, a CEO/board member of several small companies, including one public company (Portage Biotech).
Joanna Vitfell-Rasmussen, Stan Kaye, Samir Undevia, Ahmad Awada and other authors report no conflict of interest/disclosure.
Figures

References
-
- Bhide RS, Lombardo LJ, Hunt JT, et al. The antiangiogenic activity in xenograft models of brivanib, a dual inhibitor of vascular endothelial growth factor receptor-2 and fibroblast growth factor receptor-1 kinases. Mol Cancer Ther 2010;9(2):369–78. - PubMed
-
- Cai ZW, Zhang Y, Borzilleri RM, et al. Discovery of brivanib alaninate ((S)-((R)-1-(4-(4-fluoro-2-methyl-1H-indol-5-yloxy)-5methylpyrrolo[2,1-f][1,2,4] triazin-6-yloxy)propan-2-yl)2-aminopropanoate), a novel prodrug of dual vascular endothelial growth factor receptor-2 and fibroblast growth factor receptor-1 kinase inhibitor (BMS-540215). J Med Chem 2008;51(6):1976–80. - PubMed
-
- Ahmad I, Iwata T, Leung HY. Mechanisms of FGFR-mediated carcinogenesis. Biochim Biophys Acta 2012;1823(4):850–60. - PubMed
-
- Platero S, Mokliatchouk O, Jayson GC, et al. Correlation of FGF2 tumor expression with tumor response, PFS and changes in plasma pharmacodynamics markers following treatment with brivanib alaninate, an oral dual inhibitor of VEGFR FGFR tyrosine kinases. J Clin Oncol 2008;26(15S):3506.
-
- Ratain MJ, Eisen T, Stadler WM, et al. Phase II placebo-controlled randomized discontinuation trial of sorafenib in patients with metastatic renal cell carcinoma. J Clin Oncol 2006; 24(16):2505–12. - PubMed
