

Sustained outcomes in oral immunotherapy for peanut allergy (POISED study): a large, randomised, double-blind, placebo-controlled, phase 2 study
- PMID: 31522849
- PMCID: PMC6903389
- DOI: 10.1016/S0140-6736(19)31793-3
Sustained outcomes in oral immunotherapy for peanut allergy (POISED study): a large, randomised, double-blind, placebo-controlled, phase 2 study
Erratum in
-
Department of Error.Lancet. 2020 Aug 8;396(10248):380. doi: 10.1016/S0140-6736(20)31570-1. Lancet. 2020. PMID: 32771105 No abstract available.
Abstract
Background: Dietary avoidance is recommended for peanut allergies. We evaluated the sustained effects of peanut allergy oral immunotherapy (OIT) in a randomised long-term study in adults and children.
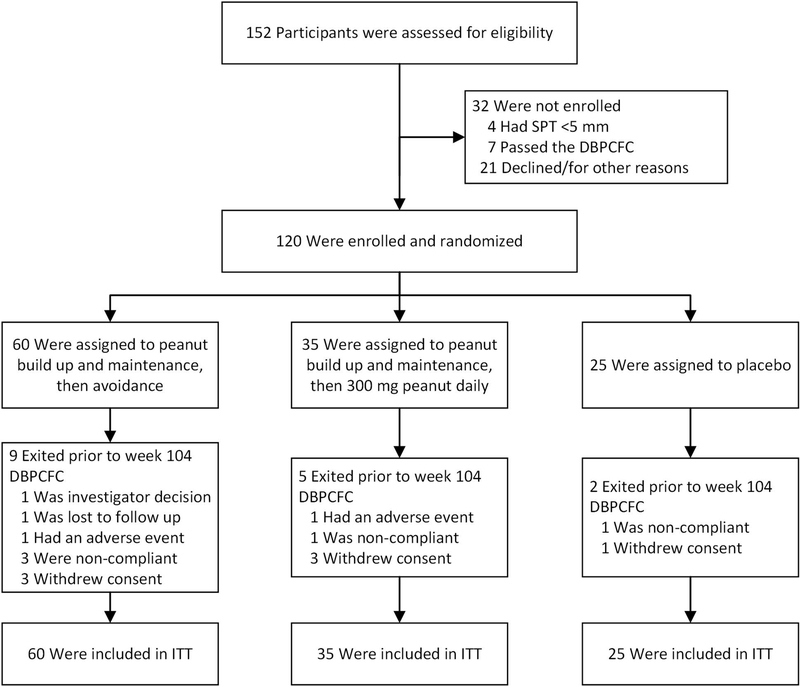
Methods: In this randomised, double-blind, placebo-controlled, phase 2 study, we enrolled participants at the Sean N Parker Center for Allergy and Asthma Research at Stanford University (Stanford, CA, USA) with peanut allergy aged 7-55 years with a positive result from a double-blind, placebo-controlled, food challenge (DBPCFC; ≤500 mg of peanut protein), a positive skin-prick test (SPT) result (≥5 mm wheal diameter above the negative control), and peanut-specific immunoglobulin (Ig)E concentration of more than 4 kU/L. Participants were randomly assigned (2·4:1·4:1) in a two-by-two block design via a computerised system to be built up and maintained on 4000 mg peanut protein through to week 104 then discontinued on peanut (peanut-0 group), to be built up and maintained on 4000 mg peanut protein through to week 104 then to ingest 300 mg peanut protein daily (peanut-300 group) for 52 weeks, or to receive oat flour (placebo group). DBPCFCs to 4000 mg peanut protein were done at baseline and weeks 104, 117, 130, 143, and 156. The pharmacist assigned treatment on the basis of a randomised computer list. Peanut or placebo (oat) flour was administered orally and participants and the study team were masked throughout by use of oat flour that was similar in look and feel to the peanut flour and nose clips, as tolerated, to mask taste. The statistician was also masked. The primary endpoint was the proportion of participants who passed DBPCFCs to a cumulative dose of 4000 mg at both 104 and 117 weeks. The primary efficacy analysis was done in the intention-to-treat population. Safety was assessed in the intention-to-treat population. This trial is registered at ClinicalTrials.gov, NCT02103270.
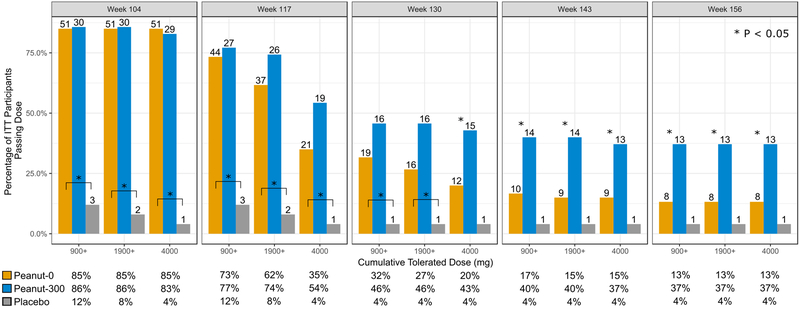
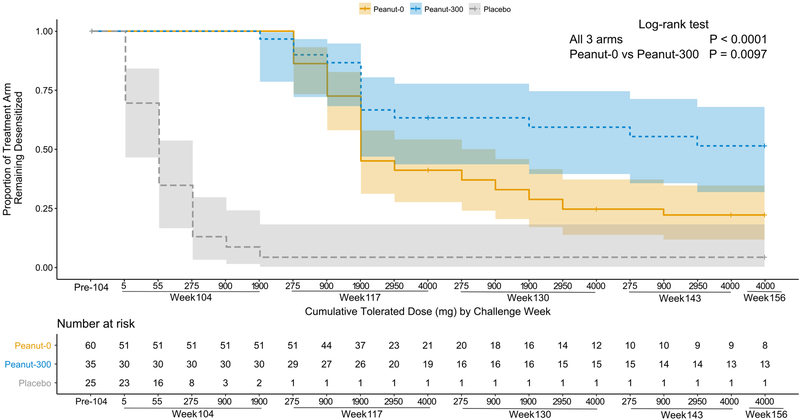
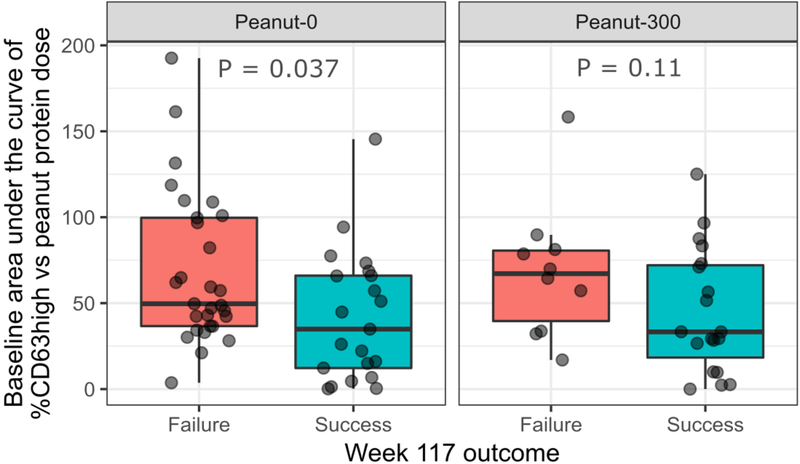
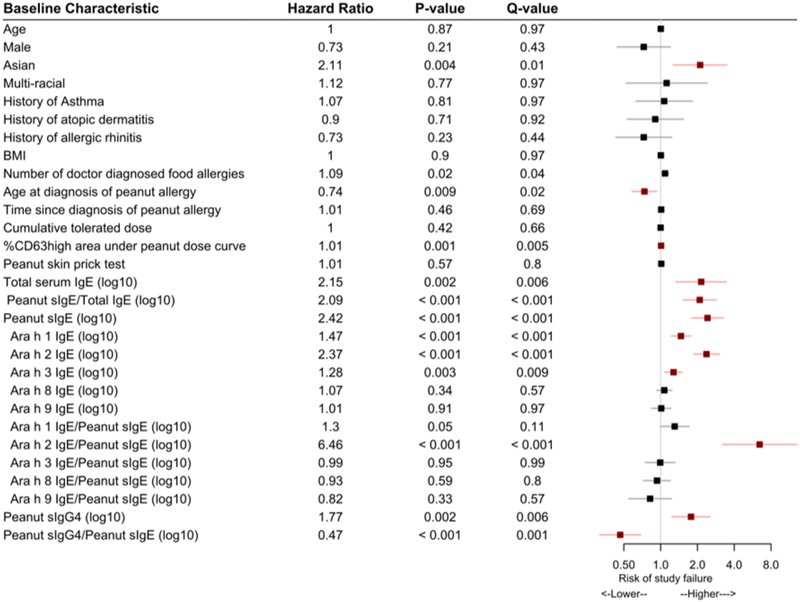
Findings: Between April 15, 2014, and March 2, 2016, of 152 individuals assessed, we enrolled 120 participants, who were randomly assigned to the peanut-0 (n=60), peanut-300 (n=35), and placebo groups (n=25). 21 (35%) of peanut-0 group participants and one (4%) placebo group participant passed the 4000 mg challenge at both 104 and 117 weeks (odds ratio [OR] 12·7, 95% CI 1·8-554·8; p=0·0024). Over the entire study, the most common adverse events were mild gastrointestinal symptoms, which were seen in 90 of 120 patients (50/60 in the peanut-0 group, 29/35 in the peanut-300 group, and 11/25 in the placebo group) and skin disorders, which were seen in 50/120 patients (26/60 in the peanut-0 group, 15/35 in the peanut-300 group, and 9/25 in the placebo group). Adverse events decreased over time in all groups. Two participants in the peanut groups had serious adverse events during the 3-year study. In the peanut-0 group, in which eight (13%) of 60 participants passed DBPCFCs at week 156, higher baseline peanut-specific IgG4 to IgE ratio and lower Ara h 2 IgE and basophil activation responses were associated with sustained unresponsiveness. No treatment-related deaths occurred.
Interpretation: Our study suggests that peanut OIT could desensitise individuals with peanut allergy to 4000 mg peanut protein but discontinuation, or even reduction to 300 mg daily, could increase the likelihood of regaining clinical reactivity to peanut. Since baseline blood tests correlated with week 117 treatment outcomes, this study might aid in optimal patient selection for this therapy.
Funding: National Institute of Allergy and Infectious Diseases.
Copyright © 2019 Elsevier Ltd. All rights reserved.
Conflict of interest statement
DECLARATION OF INTERESTS
Dr. Kari Nadeau: NIAID CoFAR, NIAID Immune Tolerance Network, NHLBI Data and Safety Monitoring Board, NIAID grant awardee, NHLBI grant awardee, NIEHS grant awardee, EPA grant awardee, FARE Center of Excellence Director, WAO Center of Excellence Director, sponsored research for clinical studies from Aimmune, DBV, AnaptysBio, Astellas, Novartis, Regeneron, Adare, Sanofi, Stallergenes-Greer. Dr. Sharon Chinthrajah receives grant support from CoFAR NIAID, Aimmune, DBV Technologies, Astellas, AnaptysBio, Novartis, Regeneron, Stallergenes-Greer, and Boehringer Ingelheim, and is a scientific advisory board member for Alladapt Immunotherapeutics. Dr. Stephen J. Galli receives grant support from NIAID, NIAMS, and the Tobacco-Related Disease Research Program (U. California). Dr. Scott Boyd receives grant support from NIAID, has been an expert witness in a patent lawsuit involving Amgen, Regeneron and Sanofi, and is a scientific advisory board member for the Food Allergy Fund. Dr. Holden Maecker receives grant support from NIAID and Amgen.
Figures
Comment in
-
Sustained unresponsiveness in peanut oral immunotherapy.Lancet. 2019 Oct 19;394(10207):1392-1393. doi: 10.1016/S0140-6736(19)31816-1. Epub 2019 Sep 12. Lancet. 2019. PMID: 31522848 No abstract available.
References
-
- Gupta RS, Springston EE, Warrier MR, et al. The prevalence, severity, and distribution of childhood food allergy in the United States. Pediatrics 2011;128:e9–17. - PubMed
-
- Feuille E, Nowak-Wegrzyn A. Oral Immunotherapy for Food Allergies. Ann Nutr Metab 2016;68 Suppl 1:19–31. - PubMed
-
- Palisade Group of Clinical Investigators. AR101 Oral Immunotherapy for Peanut Allergy. N Engl J Med 2018;379:1991–2001. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
