

Serotonin Syndrome: Pathophysiology, Clinical Features, Management, and Potential Future Directions
- PMID: 31523132
- PMCID: PMC6734608
- DOI: 10.1177/1178646919873925
Serotonin Syndrome: Pathophysiology, Clinical Features, Management, and Potential Future Directions
Abstract
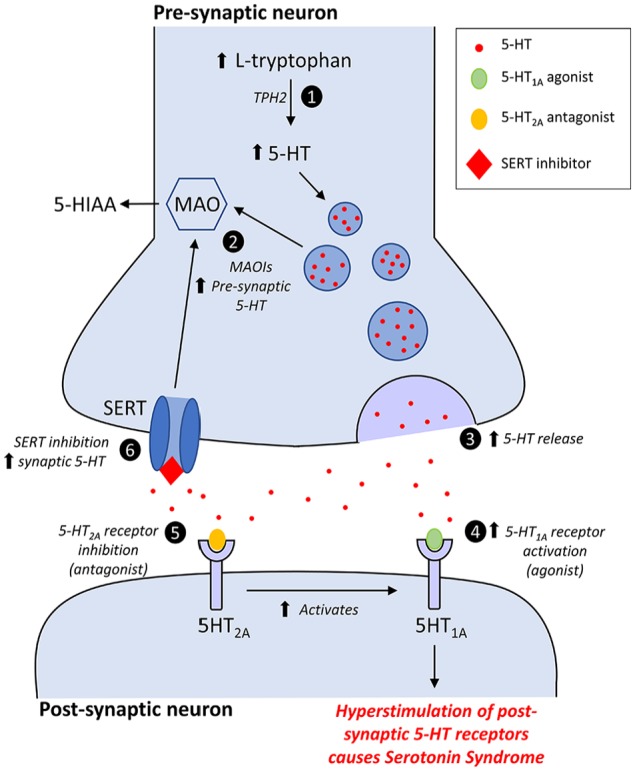
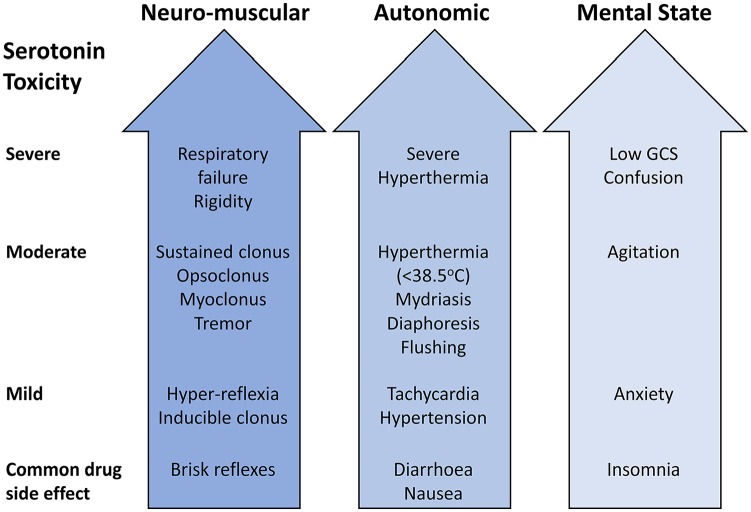
Serotonin syndrome (SS) (also referred to as serotonin toxicity) is a potentially life-threatening drug-induced toxidrome associated with increased serotonergic activity in both the peripheral (PNS) and central nervous systems (CNS). It is characterised by a dose-relevant spectrum of clinical findings related to the level of free serotonin (5-hydroxytryptamine [5-HT]), or 5-HT receptor activation (predominantly the 5-HT1A and 5-HT2A subtypes), which include neuromuscular abnormalities, autonomic hyperactivity, and mental state changes. Severe SS is only usually precipitated by the simultaneous initiation of 2 or more serotonergic drugs, but the syndrome can also occur after the initiation of a single serotonergic drug in a susceptible individual, the addition of a second or third agent to long-standing doses of a maintenance serotonergic drug, or after an overdose. The combination of a monoamine oxidase inhibitor (MAOI), in particular MAO-A inhibitors that preferentially inhibit the metabolism of 5-HT, with serotonergic drugs is especially dangerous, and may lead to the most severe form of the syndrome, and occasionally death. This review describes our current understanding of the pathophysiology, clinical presentation and management of SS, and summarises some of the drugs and interactions that may precipitate the condition. We also discuss the newer novel psychoactive substances (NPSs), a growing public health concern due to their increased availability and use, and their potential risk to evoke the syndrome. Finally, we discuss whether the inhibition of tryptophan hydroxylase (TPH), in particular the neuronal isoform (TPH2), may provide an opportunity to pharmacologically target central 5-HT synthesis, and so develop new treatments for severe, life-threatening SS.
Keywords: Serotonin syndrome; neuroleptic malignant syndrome; novel psychoactive substances; serotonin toxicity; toxidromes; tryptophan hydroxylase inhibitors.
Conflict of interest statement
Declaration of conflicting interests:The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
Comment in
-
Utilization patterns, cardiovascular risk, and concomitant serotoninergic medications among triptan users between 2008 and 2018: A gender analysis in one Italian region, Tuscany.Headache. 2023 Feb;63(2):222-232. doi: 10.1111/head.14463. Epub 2023 Jan 27. Headache. 2023. PMID: 36705316
References
-
- Eadie MJ. Convulsive ergotism: epidemics of the serotonin syndrome. Lancet Neurol. 2003;2:429-434. - PubMed
-
- Rapport MM, Green AA, Page IH. Serum vasoconstrictor, serotonin: isolation and characterization. J Biol Chem. 1948;176:1243-1251. - PubMed
-
- Oates JA, Sjoerdsma A. Neurologic effects of tryptophan in patients receiving a monoamine oxidase inhibitor. Neurology. 1960;10:1076-1078. - PubMed
-
- Gerson SC, Baldessarini RJ. Motor effects of serotonin in the central nervous system. Life Sci. 1980;27:1435-1451. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Medical
