

Prehospital plasma in injured patients is associated with survival principally in blunt injury: Results from two randomized prehospital plasma trials
- PMID: 31524836
- PMCID: PMC6923541
- DOI: 10.1097/TA.0000000000002485
Prehospital plasma in injured patients is associated with survival principally in blunt injury: Results from two randomized prehospital plasma trials
Abstract
Introduction: Recent evidence demonstrated that prehospital plasma in patients at risk of hemorrhagic shock was safe for ground transport and resulted in a 28-day survival benefit for air medical transport patients. Whether any beneficial effect of prehospital plasma varies across injury mechanism remains unknown.
Methods: We performed a secondary analysis using a harmonized data set derived from two recent prehospital plasma randomized trials. Identical inclusion/exclusion criteria and primary/secondary outcomes were used for the trials. Prehospital time, arrival shock parameters, and 24-hour transfusion requirements were compared across plasma and control groups stratified by mechanism of injury. Stratified survival analysis and Cox hazard regression were performed to determine the independent survival benefits of plasma across blunt and penetrating injury.
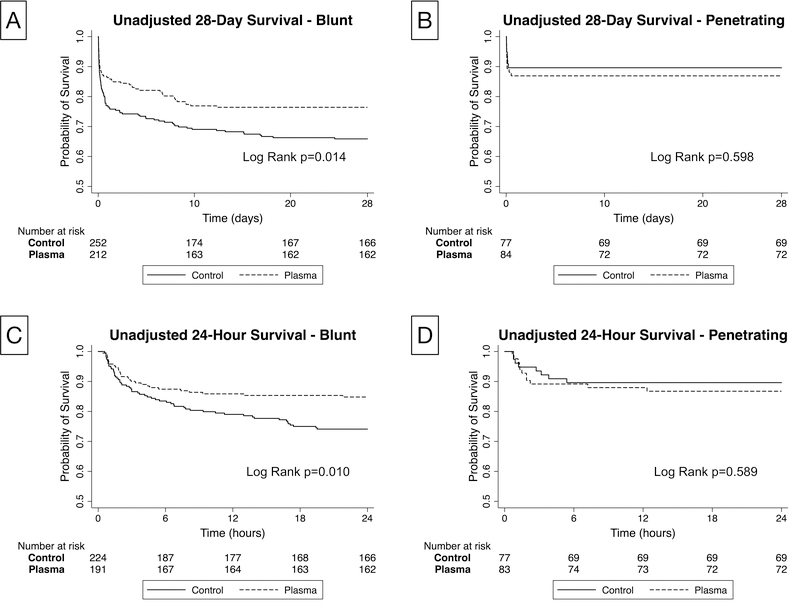
Results: Blunt patients had higher injury severity, were older, and had a lower Glasgow Coma Scale. Arrival indices of shock and coagulation parameters were similar across blunt and penetrating injury. The percentage of patients with a prehospital time less than 20 minutes was significantly higher for penetrating patients relative to blunt injured patients (28.0% vs. 11.6%, p < 0.01). Stratified Kaplan-Meier curves demonstrated a significant separation for blunt injured patients (n = 465, p = 0.01) with no separation demonstrated for penetrating injured patients (n = 161, p = 0.60) Stratified Cox hazard regression verified, after controlling for all important confounders, that prehospital plasma was associated with a 32% lower independent hazard for 28-day mortality in blunt injured patients (hazard ratio, 0.68; 95% confidence interval, 0.47-0.96; p = 0.03) with no independent survival benefit found in penetrating patients (hazard ratio, 1.16; 95% confidence interval, 0.4-3.1; p = 0.78).
Conclusion: A survival benefit associated with prehospital plasma at 24 hours and 28 days exists primarily in blunt injured patients with no benefit shown in penetrating trauma patients. No detrimental effects attributable to plasma are demonstrated in penetrating injury. These results have important relevance to military and civilian trauma systems.
Level of evidence: Therapeutic, I.
Conflict of interest statement
Figures
Similar articles
-
Severity of hemorrhage and the survival benefit associated with plasma: Results from a randomized prehospital plasma trial.J Trauma Acute Care Surg. 2020 Jan;88(1):141-147. doi: 10.1097/TA.0000000000002530. J Trauma Acute Care Surg. 2020. PMID: 31688793 Clinical Trial.
-
Forgot calcium? Admission ionized-calcium in two civilian randomized controlled trials of prehospital plasma for traumatic hemorrhagic shock.J Trauma Acute Care Surg. 2020 May;88(5):588-596. doi: 10.1097/TA.0000000000002614. J Trauma Acute Care Surg. 2020. PMID: 32317575 Free PMC article. Clinical Trial.
-
Survival bias in pediatric hemorrhagic shock: Are we misrepresenting the data?J Trauma Acute Care Surg. 2024 May 1;96(5):785-792. doi: 10.1097/TA.0000000000004119. Epub 2023 Sep 27. J Trauma Acute Care Surg. 2024. PMID: 37752639
-
Permissive hypotension versus conventional resuscitation strategies in adult trauma patients with hemorrhagic shock: A systematic review and meta-analysis of randomized controlled trials.J Trauma Acute Care Surg. 2018 May;84(5):802-808. doi: 10.1097/TA.0000000000001816. J Trauma Acute Care Surg. 2018. PMID: 29370058
-
Prehospital fluid resuscitation in hypotensive trauma patients: do we need a tailored approach?Injury. 2015 Jan;46(1):4-9. doi: 10.1016/j.injury.2014.08.001. Epub 2014 Aug 11. Injury. 2015. PMID: 25173671 Review.
Cited by
-
Mechanism matters: mortality and endothelial cell damage marker differences between blunt and penetrating traumatic injuries across three prehospital clinical trials.Sci Rep. 2024 Feb 2;14(1):2747. doi: 10.1038/s41598-024-53398-1. Sci Rep. 2024. PMID: 38302619 Free PMC article.
-
Association of red blood cells and plasma transfusion versus red blood cell transfusion only with survival for treatment of major traumatic hemorrhage in prehospital setting in England: a multicenter study.Crit Care. 2023 Jan 17;27(1):25. doi: 10.1186/s13054-022-04279-4. Crit Care. 2023. PMID: 36650557 Free PMC article.
-
[Prehospital blood transfusion : Opportunities and challenges for the German emergency medical services].Anaesthesiologie. 2024 Nov;73(11):760-770. doi: 10.1007/s00101-024-01463-9. Epub 2024 Oct 2. Anaesthesiologie. 2024. PMID: 39356309 Free PMC article. Review. German.
-
Prehospital Lyophilized Plasma Transfusion for Trauma-Induced Coagulopathy in Patients at Risk for Hemorrhagic Shock: A Randomized Clinical Trial.JAMA Netw Open. 2022 Jul 1;5(7):e2223619. doi: 10.1001/jamanetworkopen.2022.23619. JAMA Netw Open. 2022. PMID: 35881397 Free PMC article. Clinical Trial.
-
The efficacy and safety of pre-hospital plasma in patients at risk for hemorrhagic shock: an updated systematic review and meta-analysis of randomized controlled trials.Eur J Trauma Emerg Surg. 2024 Dec;50(6):2697-2707. doi: 10.1007/s00068-024-02461-7. Epub 2024 Feb 17. Eur J Trauma Emerg Surg. 2024. PMID: 38367091 Free PMC article.
References
-
- Cotton BA, Reddy N, Hatch QM, LeFebvre E, Wade CE, Kozar RA, Gill BS, Albarado R, McNutt MK, Holcomb JB. Damage control resuscitation is associated with a reduction in resuscitation volumes and improvement in survival in 390 damage control laparotomy patients. Ann Surg. 2011;254(4):598–605. - PMC - PubMed
-
- Harris T, Davenport R, Mak M, Brohi K. The Evolving Science of Trauma Resuscitation. Emerg Med Clin North Am. 2018;36(1):85–106. - PubMed
-
- Holcomb JB, del Junco DJ, Fox EE, Wade CE, Cohen MJ, Schreiber MA, Alarcon LH, Bai Y, Brasel KJ, Bulger EM, et al. The prospective, observational, multicenter, major trauma transfusion (PROMMTT) study: comparative effectiveness of a time-varying treatment with competing risks. JAMA Surg. 2013;148(2):127–36. - PMC - PubMed
-
- Holcomb JB, Tilley BC, Baraniuk S, Fox EE, Wade CE, Podbielski JM, del Junco DJ, Brasel KJ, Bulger EM, Callcut RA, et al. Transfusion of plasma, platelets, and red blood cells in a 1:1:1 vs a 1:1:2 ratio and mortality in patients with severe trauma: the PROPPR randomized clinical trial. JAMA. 2015;313(5):471–82. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
