

Fast and near-optimal monitoring for healthcare acquired infection outbreaks
- PMID: 31525183
- PMCID: PMC6762212
- DOI: 10.1371/journal.pcbi.1007284
Fast and near-optimal monitoring for healthcare acquired infection outbreaks
Abstract
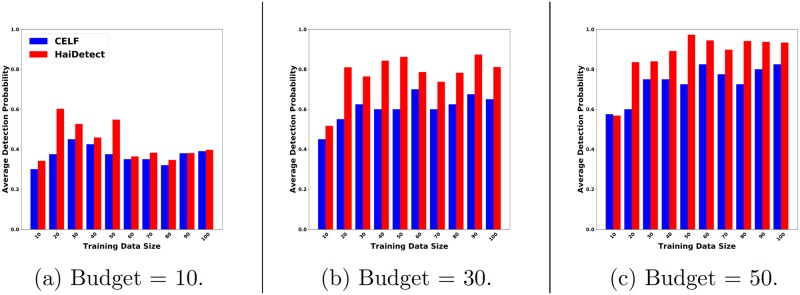
According to the Centers for Disease Control and Prevention (CDC), one in twenty five hospital patients are infected with at least one healthcare acquired infection (HAI) on any given day. Early detection of possible HAI outbreaks help practitioners implement countermeasures before the infection spreads extensively. Here, we develop an efficient data and model driven method to detect outbreaks with high accuracy. We leverage mechanistic modeling of C. difficile infection, a major HAI disease, to simulate its spread in a hospital wing and design efficient near-optimal algorithms to select people and locations to monitor using an optimization formulation. Results show that our strategy detects up to 95% of "future" C. difficile outbreaks. We design our method by incorporating specific hospital practices (like swabbing for infections) as well. As a result, our method outperforms state-of-the-art algorithms for outbreak detection. Finally, a qualitative study of our result shows that the people and locations we select to monitor as sensors are intuitive and meaningful.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures











References
-
- Cassini A., Plachouras D., Eckmanns T., Sin M. A., Blank H.-P., Ducomble T., Haller S., Harder T., Klingeberg A., Sixtensson M., et al., “Burden of six healthcare-associated infections on european population health: estimating incidence-based disability-adjusted life years through a population prevalence-based modelling study,” PLoS medicine, vol. 13, no. 10, p. e1002150, 2016. 10.1371/journal.pmed.1002150 - DOI - PMC - PubMed
-
- Lofgren E. T., Moehring R. W., Anderson D. J., Weber D. J., and Fefferman N. H., “A mathematical model to evaluate the routine use of fecal microbiota transplantation to prevent incident and recurrent clostridium difficile infection,” Infection Control and Hospital Epidemiology, 2013. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
