

Impact of traffic variability on geographic accessibility to 24/7 emergency healthcare for the urban poor: A GIS study in Dhaka, Bangladesh
- PMID: 31525226
- PMCID: PMC6746363
- DOI: 10.1371/journal.pone.0222488
Impact of traffic variability on geographic accessibility to 24/7 emergency healthcare for the urban poor: A GIS study in Dhaka, Bangladesh
Abstract
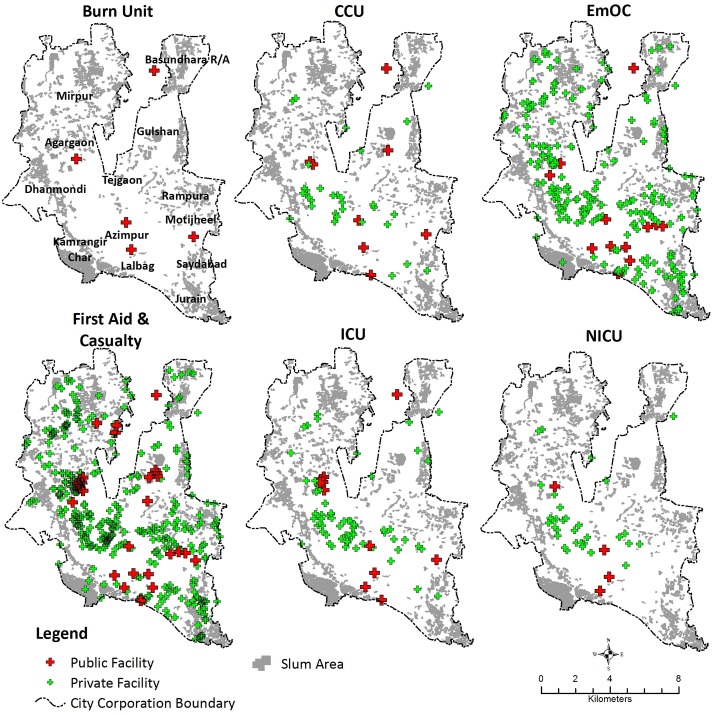
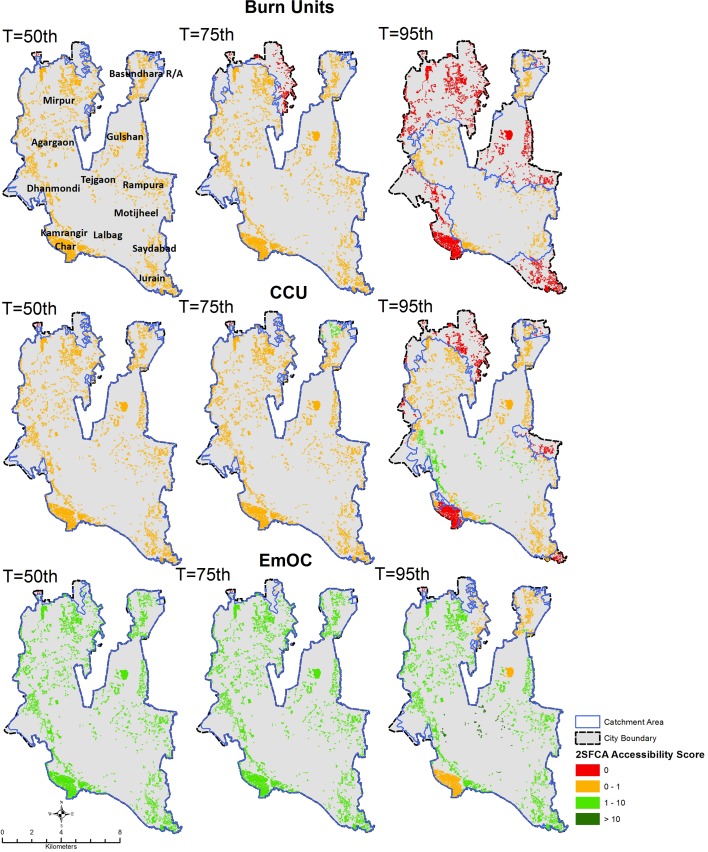
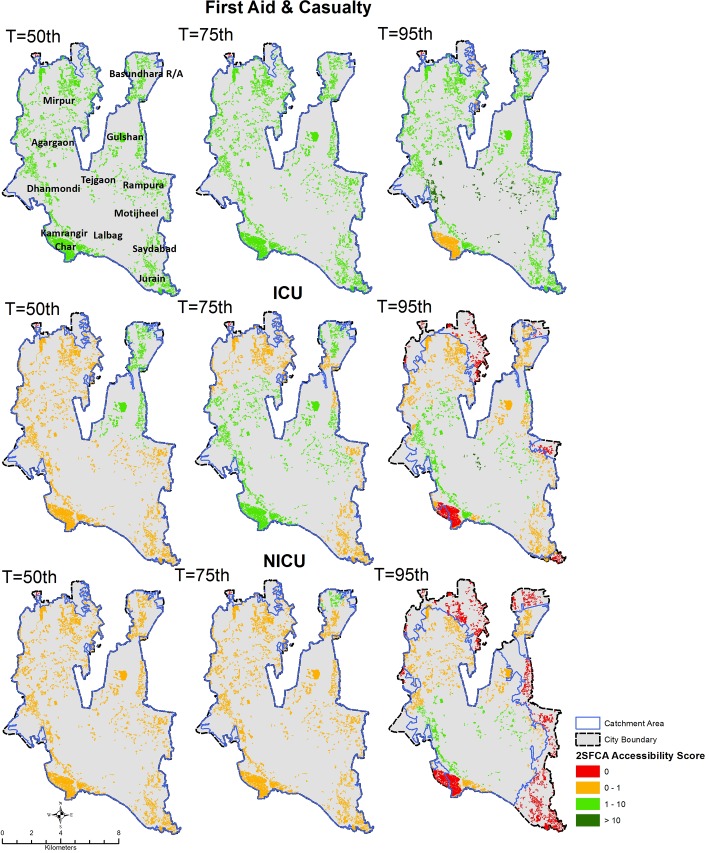
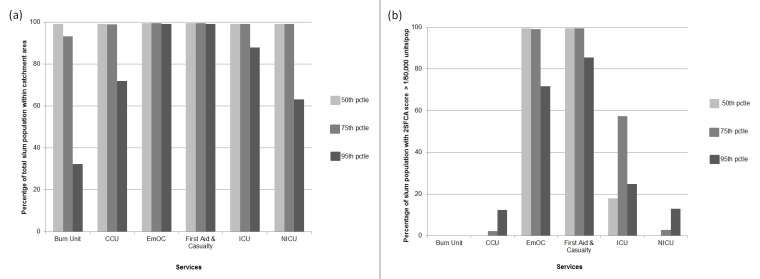
Ensuring access to healthcare in emergency health situations is a persistent concern for health system planners. Emergency services, including critical care units for severe burns and coronary events, are amongst those for which travel time is the most crucial, potentially making a difference between life and death. Although it is generally assumed that access to healthcare is not an issue in densely populated urban areas due to short distances, we prove otherwise by applying improved methods of assessing accessibility to emergency services by the urban poor that take traffic variability into account. Combining unique data on emergency health service locations, traffic flow variability and informal settlements boundaries, we generated time-cost based service areas to assess the extent to which emergency health services are reachable by urban slum dwellers when realistic traffic conditions and their variability in time are considered. Variability in traffic congestion is found to have significant impact on the measurement of timely access to, and availability of, healthcare services for slum populations. While under moderate traffic conditions all slums in Dhaka City are within 60-minutes travel time from an emergency service, in congested traffic conditions only 63% of the city's slum population is within 60-minutes reach of most emergency services, and only 32% are within 60-minutes reach of a Burn Unit. Moreover, under congested traffic conditions only 12% of slums in Dhaka City Corporation comply with Bangladesh's policy guidelines that call for access to 1 health service per 50,000 population for most emergency service types, and not a single slum achieved this target for Burn Units. Emergency Obstetric Care (EmOC) and First Aid & Casualty services provide the best coverage, with nearly 100% of the slum population having timely access within 60-minutes in any traffic condition. Ignoring variability in traffic conditions results in a 3-fold overestimation of geographic coverage and masks intra-urban inequities in accessibility to emergency care, by overestimating geographic accessibility in peripheral areas and underestimating the same for central city areas. The evidence provided can help policy makers and urban planners improve health service delivery for the urban poor. We recommend that taking traffic conditions be taken into account in future GIS-based analysis and planning for healthcare service accessibility in urban areas.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Masters S, Bursteina R, Amofahb G, Abaogyec P, Kumara S, Hanlon M. Travel time to maternity care and its effect on utilization in rural Ghana: A multilevel analysis. Social Science & Medicine. 2013;93(147–154). - PubMed
-
- Gabrysch S. The influences of distance on health facility delivery in rural Zambia: London School of Hygiene & Tropical Medicine; 2010.
-
- Zegeye K, Gebeyehu A, Melese T. The Role of Geographical Access in the Utilization of Institutional Delivery Service in Rural Jimma Horro District, Southwest Ethiopia. Primary Health Care. 2014;4(1). 10.4172/2167-1079.1000152 - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
