

Interrupting providers with clinical decision support to improve care for heart failure
- PMID: 31525580
- PMCID: PMC6994190
- DOI: 10.1016/j.ijmedinf.2019.103956
Interrupting providers with clinical decision support to improve care for heart failure
Abstract
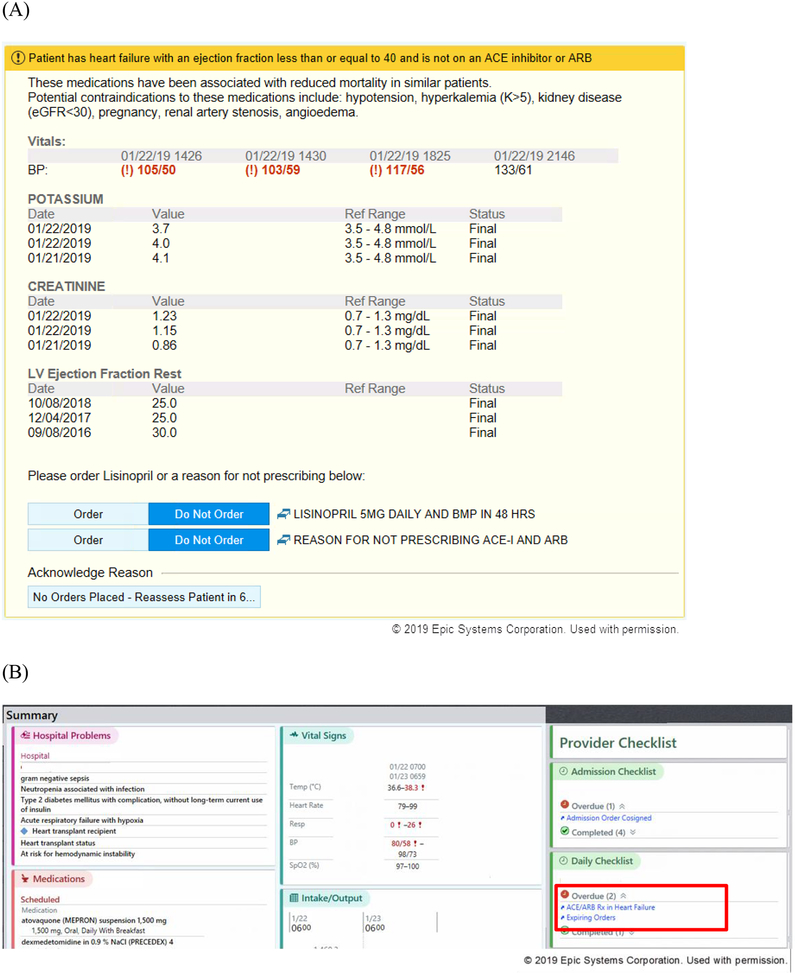
Background: Evidence-based therapy for heart failure remains underutilized at hospital discharge, particularly for patients with heart failure who are hospitalized for another cause. We developed clinical decision support (CDS) to recommend an angiotensin converting enzyme (ACE) inhibitor during hospitalization to promote its continuation at discharge. The CDS was designed to be implemented in both interruptive and non-interruptive versions.
Objectives: To compare the effectiveness and implementation of interruptive and non-interruptive versions of a CDS to improve care for heart failure.
Methods: Hospitalizations of patients with reduced ejection fraction were pseudo-randomized to deliver interruptive or non-interruptive CDS alerts to providers based on even or odd medical record number. We compared discharge utilization of an ACE inhibitor or angiotensin receptor blocker (ARB) for these two implementation approaches. We also assessed adoption and implementation fidelity of the CDS.
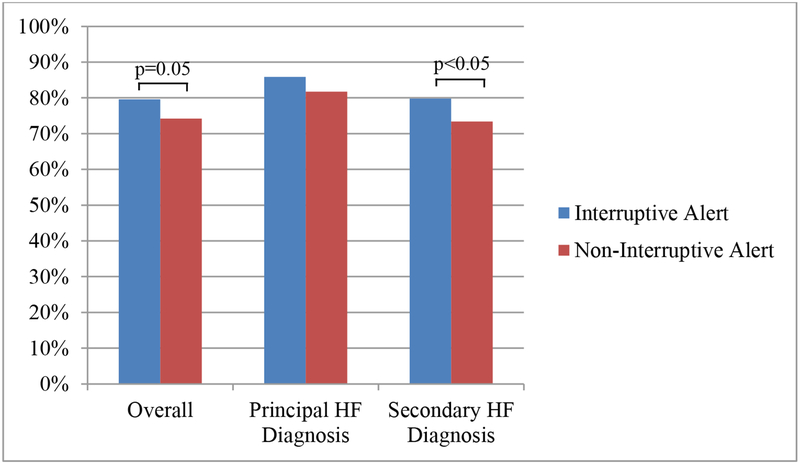
Results: Of 958 hospitalizations, interruptive alert hospitalizations had higher rates of discharge utilization of ACE inhibitors or ARBs than non-interruptive alert hospitalizations (79.6% vs. 74.2%, p = 0.05). Utilization was higher for interruptive alert versus non-interruptive alert hospitalizations which were principally for causes other than heart failure (79.8% vs. 73.4%; p = 0.05) but no difference was observed among hospitalizations with a principal heart failure diagnosis (85.9% vs.81.7%; p = 0.49). As compared to non-interruptive hospitalizations, interruptive alert hospitalizations were more likely to have had: an alert with any response (40.6% vs. 13.1%, p < 0.001), contraindications reported (33.1% vs 11.3%, p < 0.001), and an ACE inhibitor ordered within twelve hours of the alert (17.6% vs 10.3%, p < 0.01). The response rate for the interruptive alert was 1.7%, and a median (25th, 75th percentile) of 14 (5,32) alerts were triggered per hospitalization.
Conclusions: A CDS implemented as an interruptive alert was associated with improved quality of care for heart failure. Whether the potential benefits of CDS in improving cardiovascular care were worth the high burden of interruptive alerts deserves further consideration. CLINICALTRIALS.
Gov identifier: NCT02858674.
Keywords: Clinical decision support; Comparative effectiveness; Heart failure.
Copyright © 2019 Elsevier B.V. All rights reserved.
Figures
References
-
- Loehr LR, Rosamond WD, Chang PP, Folsom AR, Chambless LE. Heart failure incidence and survival (from the Atherosclerosis Risk in Communities study). The American journal of cardiology. 2008;101(7):1016–1022. - PubMed
-
- Garg R, Yusuf S. Overview of randomized trials of angiotensin-converting enzyme inhibitors on mortality and morbidity in patients with heart failure. Collaborative Group on ACE Inhibitor Trials. JAMA. 1995;273(18):1450–1456. - PubMed
-
- Yancy CW, Jessup M, Bozkurt B, et al. 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2013;62(16):e147–239. - PubMed
-
- Adams KF Jr., Fonarow GC, Emerman CL, et al. Characteristics and outcomes of patients hospitalized for heart failure in the United States: rationale, design, and preliminary observations from the first 100,000 cases in the Acute Decompensated Heart Failure National Registry (ADHERE). American heart journal. 2005;149(2):209–216. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
