

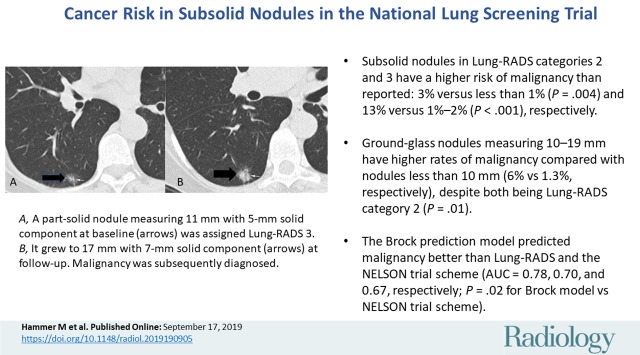
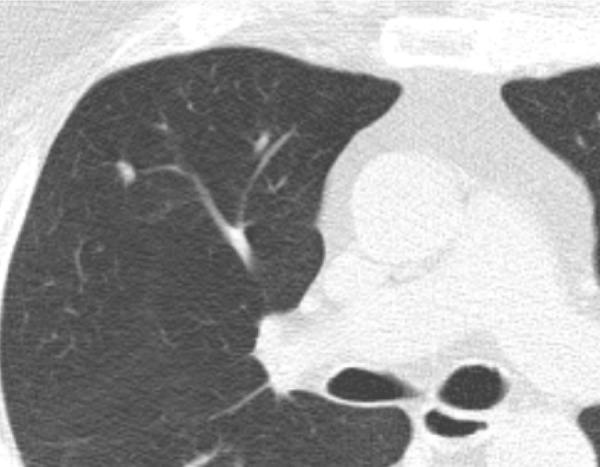
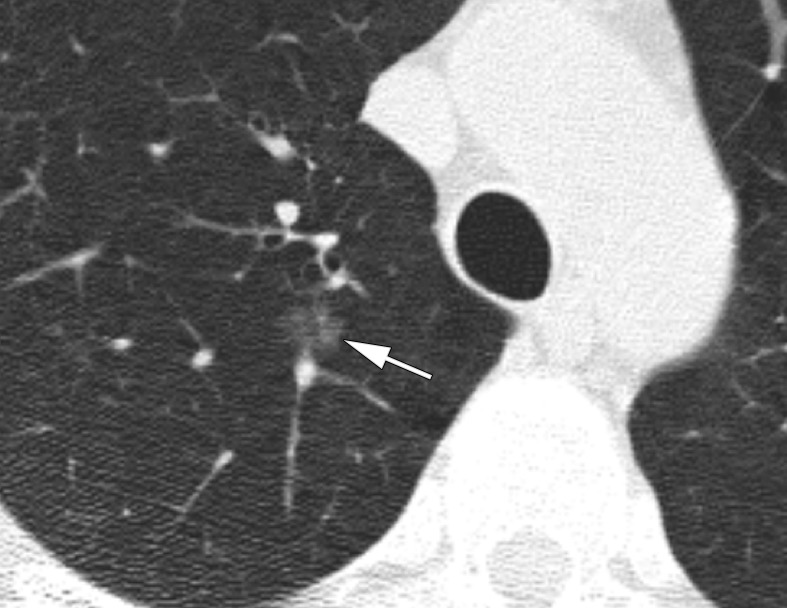
Cancer Risk in Subsolid Nodules in the National Lung Screening Trial
- PMID: 31526256
- PMCID: PMC6823608
- DOI: 10.1148/radiol.2019190905
Cancer Risk in Subsolid Nodules in the National Lung Screening Trial
Abstract
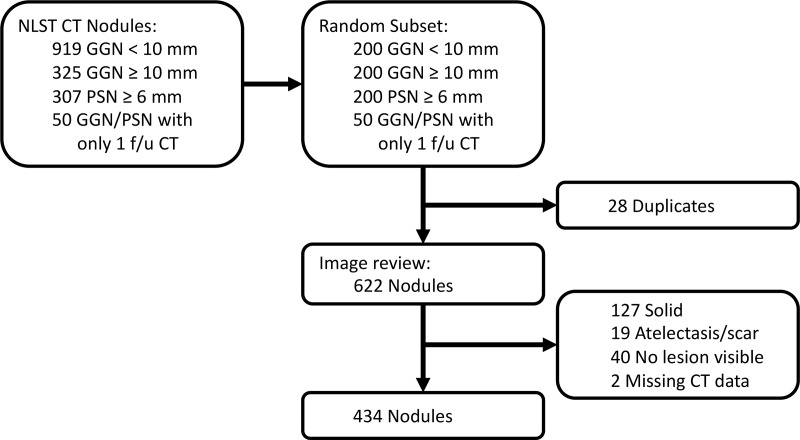
Background Subsolid pulmonary nodules, comprising pure ground-glass nodules (GGNs) and part-solid nodules (PSNs), have a high risk of indolent malignancy. Lung Imaging Reporting and Data System (Lung-RADS) nodule management guidelines are based on expert opinion and lack independent validation. Purpose To evaluate Lung-RADS estimates of the malignancy rates of subsolid nodules, using nodules from the National Lung Screening Trial (NLST), and to compare Lung-RADS to the NELSON trial classification as well as the Brock University calculator. Materials and Methods Subsets of GGNs and PSNs were selected from the NLST for this retrospective study. A thoracic radiologist reviewed the baseline and follow-up CT images, confirmed that they were true subsolid nodules, and measured the nodules. The primary outcome for each nodule was the development of malignancy within the follow-up period (median, 6.5 years). Nodules were stratified according to Lung-RADS, NELSON trial criteria, and the Brock model. For analyses, nodule subsets were weighted on the basis of frequency in the NLST data set. Nodule stratification models were tested by using receiver operating characteristic curves. Results A total of 622 nodules were evaluated, of which 434 nodules were subsolid. At baseline, 304 nodules were classified as Lung-RADS category 2, with a malignancy rate of 3%, which is greater than the 1% in Lung-RADS (P = .004). The malignancy rate for GGNs smaller than 10 mm (two of 129, 1.3%) was smaller than that for GGNs measuring 10-19 mm (11 of 153, 6%) (P = .01). The malignancy rate for Lung-RADS category 3 was 14% (13 of 67), which is greater than the reported 2% in Lung-RADS (P < .001). The Brock model predicted malignancy better than Lung-RADS and the NELSON trial scheme (area under the receiver operating characteristic curve = 0.78, 0.70, and 0.67, respectively; P = .02 for Brock model vs NELSON trial scheme). Conclusion Subsolid nodules classified as Lung Imaging Reporting and Data System (Lung-RADS) categories 2 and 3 have a higher risk of malignancy than reported. The Brock risk calculator performed better than measurement-based classification schemes such as Lung-RADS. © RSNA, 2019 Online supplemental material is available for this article. See also the editorial by Kauczor and von Stackelberg in this issue.
Figures


Comment in
-
Subsolid Lung Nodules: Potential for Overdiagnosis.Radiology. 2019 Nov;293(2):449-450. doi: 10.1148/radiol.2019191877. Epub 2019 Sep 17. Radiology. 2019. PMID: 31532302 No abstract available.
References
-
- Henschke CI, Yip R, Smith JP, et al. . CT Screening for Lung Cancer: Part-Solid Nodules in Baseline and Annual Repeat Rounds . AJR Am J Roentgenol 2016. ; 207 ( 6 ): 1176 – 1184 . - PubMed
-
- Mortani Barbosa EJ., Jr. Lung cancer screening overdiagnosis: reports of overdiagnosis in screening for lung cancer are grossly exaggerated . Acad Radiol 2015. ; 22 ( 8 ): 976 – 982 . - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
