

Pediatric postoperative cerebellar cognitive affective syndrome follows outflow pathway lesions
- PMID: 31527284
- PMCID: PMC6815203
- DOI: 10.1212/WNL.0000000000008326
Pediatric postoperative cerebellar cognitive affective syndrome follows outflow pathway lesions
Abstract
Objective: To evaluate lesion location after pediatric cerebellar tumor resection in relation to the development of severe cognitive and affective disturbances, or cerebellar cognitive affective syndrome (CCAS).
Methods: The postsurgical lesion location of 195 pediatric patients with cerebellar tumors was mapped onto a template brain. Individuals with CCAS were matched to 2 participants without CCAS by sex, age, and lesion volume. Lesion analyses included both a hypothesis-driven evaluation of the cerebellar outflow pathway (deep nuclei and superior cerebellar peduncles) and data-driven multivariate lesion symptom mapping. Lesion-associated networks were evaluated by comparing connectivity patterns between the lesion location of cases with and those without CCAS with resting-state functional connectivity MRI data from large normative adult and pediatric cohorts.
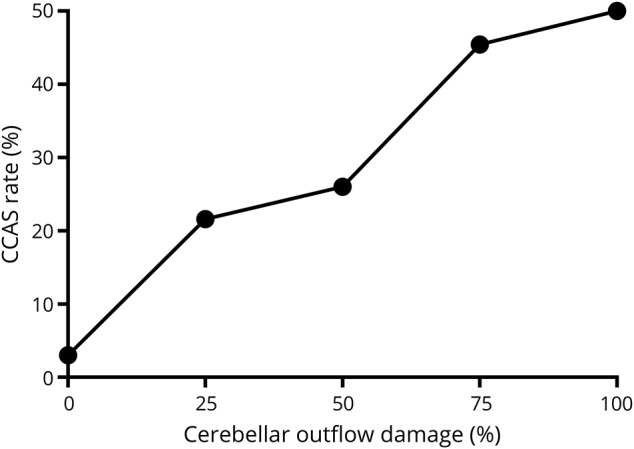
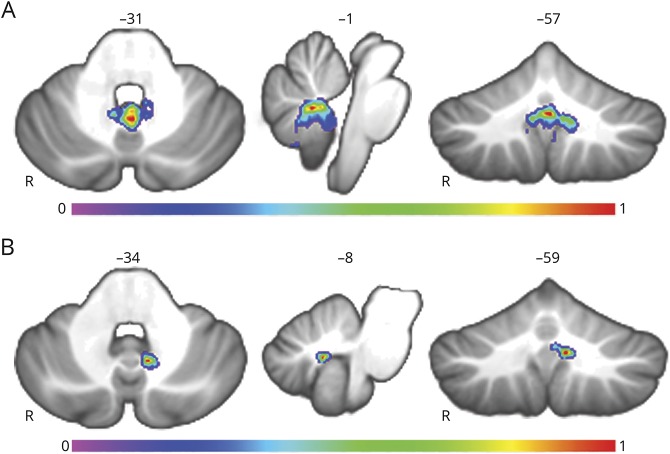
Results: CCAS was present in 48 of 195 participants (24.6%) and was strongly associated with cerebellar outflow tract lesions (p < 0.0001). Lesion symptom mapping also highlighted the cerebellar outflow pathway, with peak findings in the fastigial nuclei extending into the inferior vermis. Lesion network mapping revealed that the cerebellar region most associated with CCAS was functionally connected to the thalamic mediodorsal nucleus, among other sites, and that higher connectivity between lesion location and the mediodorsal nucleus predicts CCAS occurrence (p < 0.01). A secondary analysis of 27 participants with mutism revealed similar localization of lesions and lesion-associated networks.
Conclusion: Lesions of the cerebellar outflow pathway and inferior vermis are associated with major cognitive and affective disturbances after pediatric cerebellar tumor resection, and disrupted communication between the cerebellum and the thalamic mediodorsal nucleus may be important.
© 2019 American Academy of Neurology.
Figures





Comment in
-
Neuroanatomy of pediatric postoperative cerebellar cognitive affective syndrome and mutism.Neurology. 2019 Oct 15;93(16):693-694. doi: 10.1212/WNL.0000000000008311. Epub 2019 Sep 16. Neurology. 2019. PMID: 31527286 No abstract available.
References
-
- Lanier JC, Abrams AN. Posterior fossa syndrome: review of the behavioral and emotional aspects in pediatric cancer patients. Cancer 2017;123:551–559. - PubMed
-
- Wisoff JH, Epstein FJ. Pseudobulbar palsy after posterior fossa operation in children. Neurosurgery 1984;15:707–709. - PubMed
-
- Rekate HL, Grubb RL, Aram DM, Hahn JF, Ratcheson RA. Muteness of cerebellar origin. Arch Neurol Am Med Assoc 1985;42:697–698. - PubMed
-
- Levisohn L, Cronin-Golomb A, Schmahmann JD. Neuropsychological consequences of cerebellar tumour resection in children: cerebellar cognitive affective syndrome in a paediatric population. Brain 2000;123:1041–1050. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical