

Impact of national Human Development Index on liver cancer outcomes: Transition from 2008 to 2018
- PMID: 31528099
- PMCID: PMC6718041
- DOI: 10.3748/wjg.v25.i32.4749
Impact of national Human Development Index on liver cancer outcomes: Transition from 2008 to 2018
Abstract
Background: Liver cancer is the sixth most commonly diagnosed cancer and the fourth leading cause of cancer death worldwide. Socioeconomic development, indicated by the Human Development Index (HDI), is closely interconnected with public health. But the manner in which social development and medical advances influenced liver cancer patients in the past decade is still unknown.
Aim: To investigate the influence of HDI on clinical outcomes for patients with existing liver cancer from 2008 to 2018.
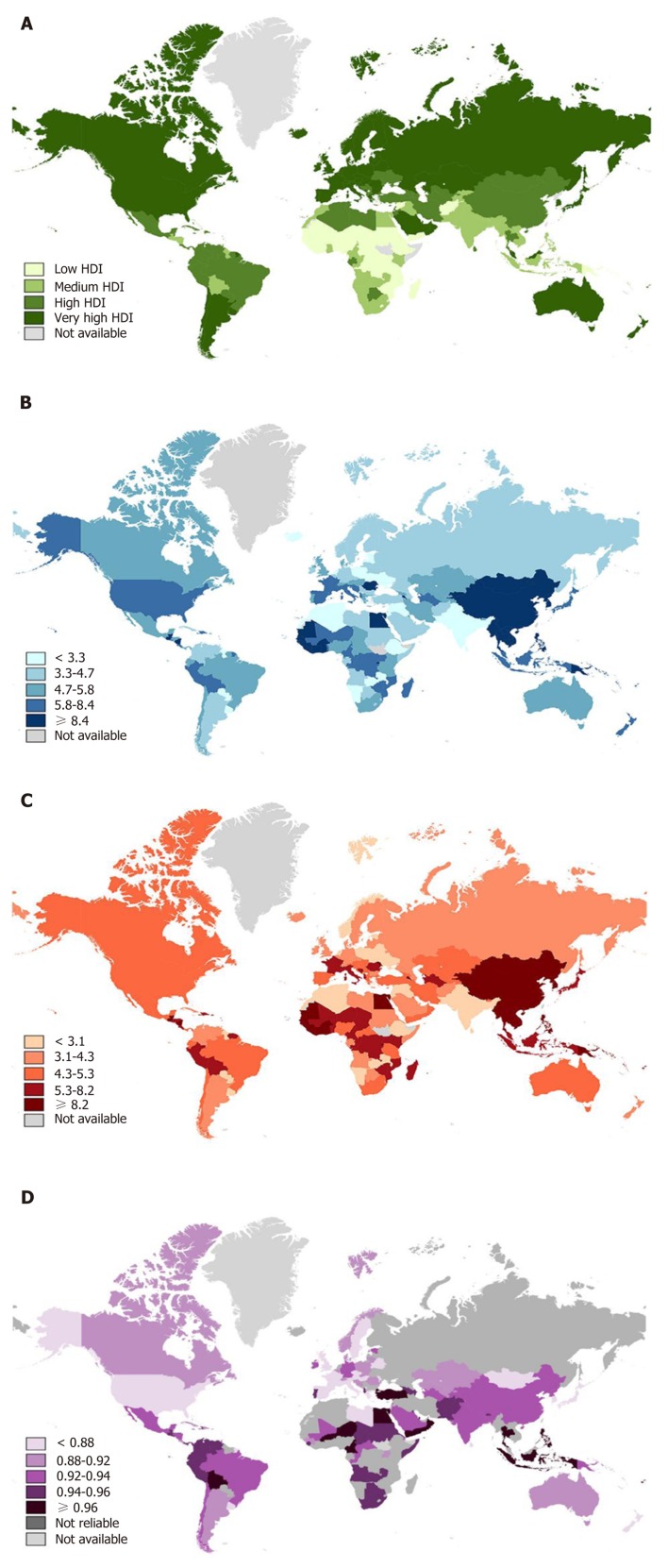
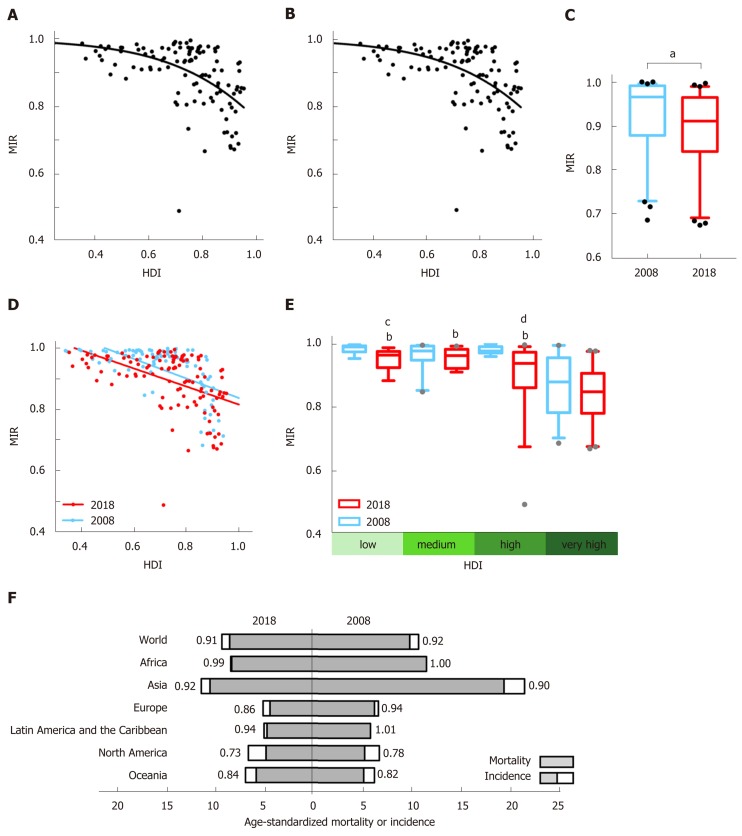
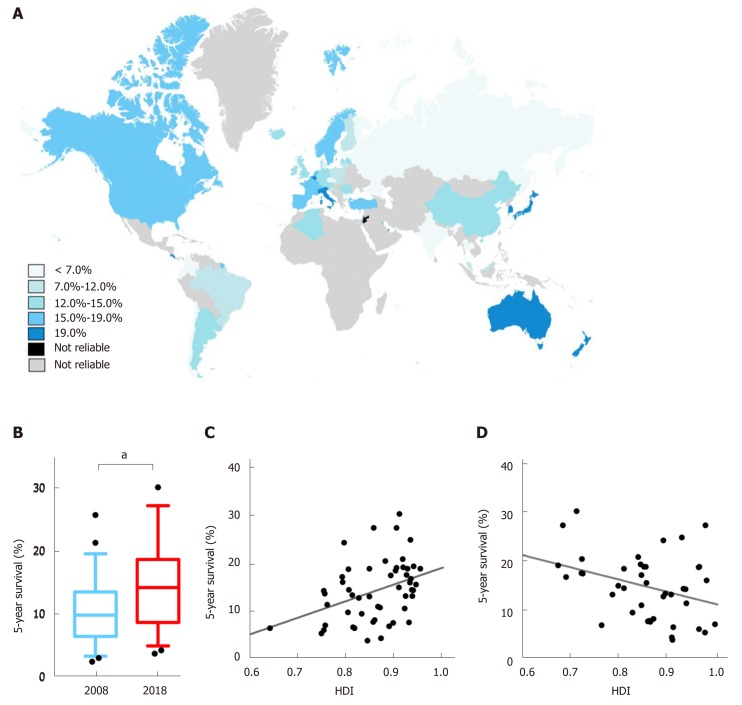
Methods: The HDI values were obtained from the United Nations Development Programme, the age-standardized incidence and mortality rates of liver cancer were obtained from the GLOBOCAN database to calculate the mortality-to-incidence ratio, and the estimated 5-year net survival of patients with liver cancer was provided by the CONCORD-3 program. We then explored the association of mortality-to-incidence ratio and survival with HDI, with a focus on geographic variability across countries as well as temporal heterogeneity over the past decade.
Results: From 2008 to 2018, the epidemiology of liver cancer had changed across countries. Liver cancer mortality-to-incidence ratios were negatively correlated and showed good fit with a modified "dose-to-inhibition response" pattern with HDI (r = -0.548, P < 0.0001 for 2018; r = -0.617, P < 0.0001 for 2008). Cancer survival was positively associated with HDI (r = 0.408, P < 0.01) and negatively associated with mortality-to-incidence ratio (r = -0.346, P < 0.05), solidly confirming the interrelation among liver cancer outcome indicators and socioeconomic factors. Notably, in the past decade, the HDI values in most countries have increased alongside a decreasing tendency of liver cancer mortality-to-incidence ratios (P < 0.0001), and survival outcomes have simultaneously improved (P < 0.001), with significant disparities across countries.
Conclusion: Socioeconomic factors have a significant influence on cancer outcomes. HDI values have increased along with improved cancer outcomes, with significant disparities among countries.
Keywords: Human Development Index; Incidence; Liver cancer; Mortality; Survival.
Conflict of interest statement
Conflict-of-interest statement: All the authors have no conflict of interest related to the manuscript.
Figures
References
-
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68:394–424. - PubMed
-
- Reis-Filho JS, Pusztai L. Gene expression profiling in breast cancer: Classification, prognostication, and prediction. Lancet. 2011;378:1812–1823. - PubMed
-
- Hirsch FR, Scagliotti GV, Mulshine JL, Kwon R, Curran WJ, Jr, Wu YL, Paz-Ares L. Lung cancer: Current therapies and new targeted treatments. Lancet. 2017;389:299–311. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
