

Prognostic models based on postoperative circulating tumor cells can predict poor tumor recurrence-free survival in patients with stage II-III colorectal cancer
- PMID: 31528219
- PMCID: PMC6746136
- DOI: 10.7150/jca.30512
Prognostic models based on postoperative circulating tumor cells can predict poor tumor recurrence-free survival in patients with stage II-III colorectal cancer
Abstract
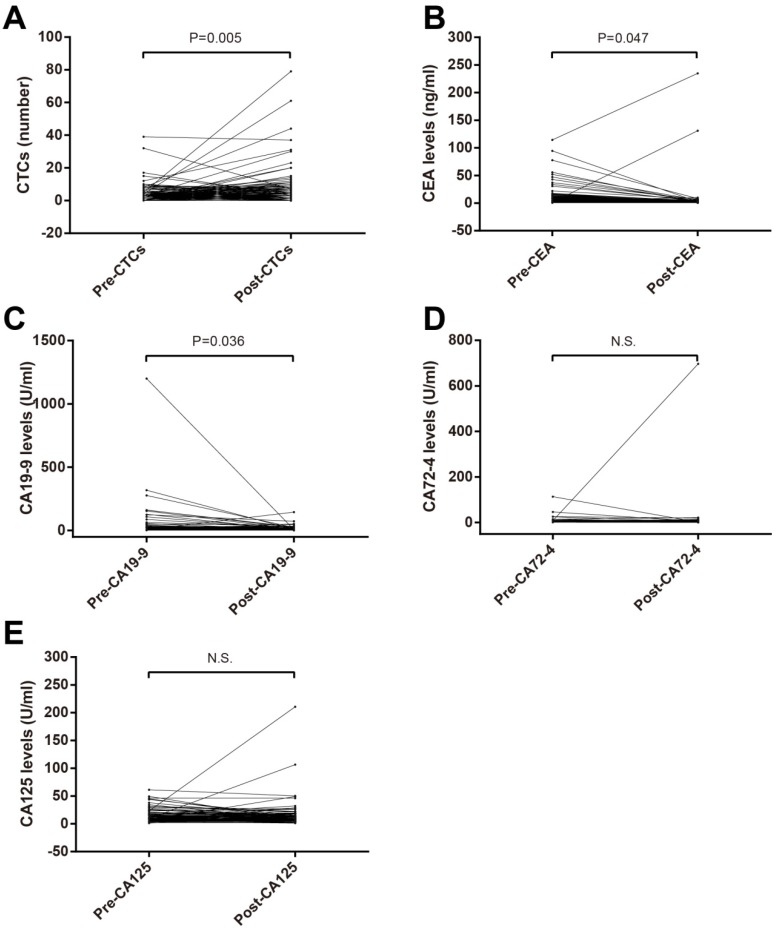
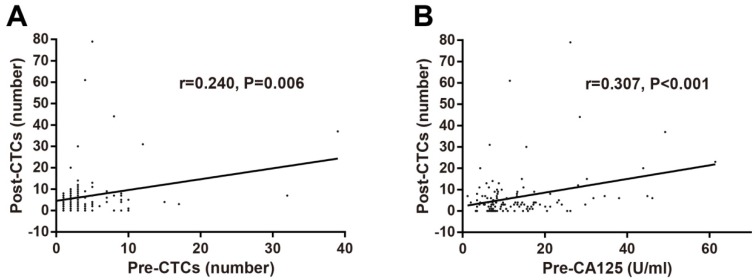
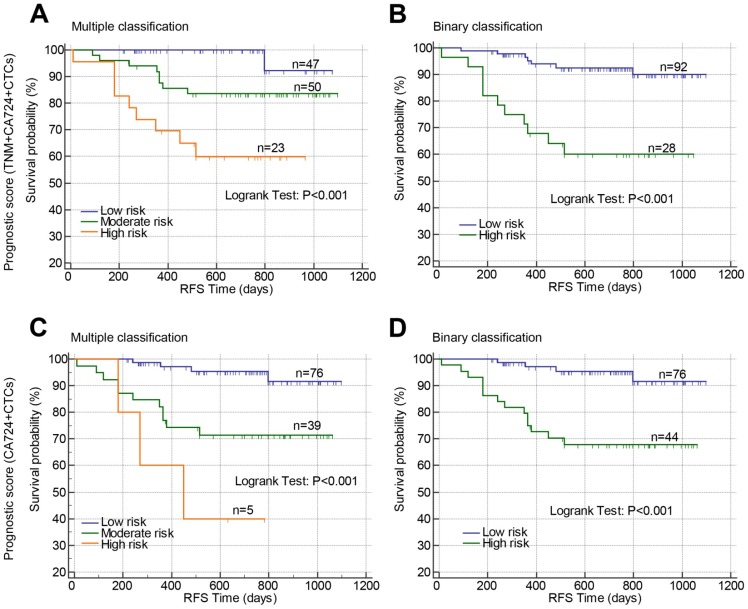
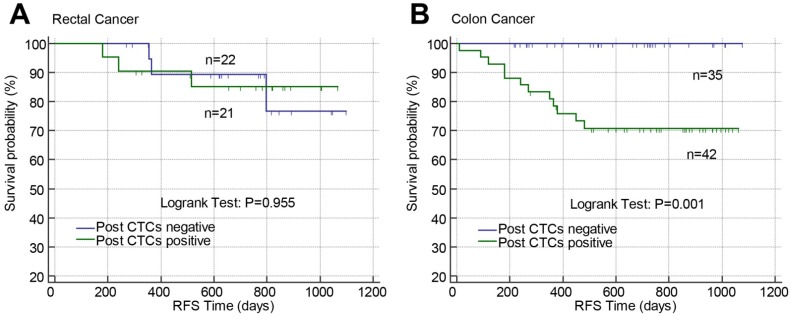
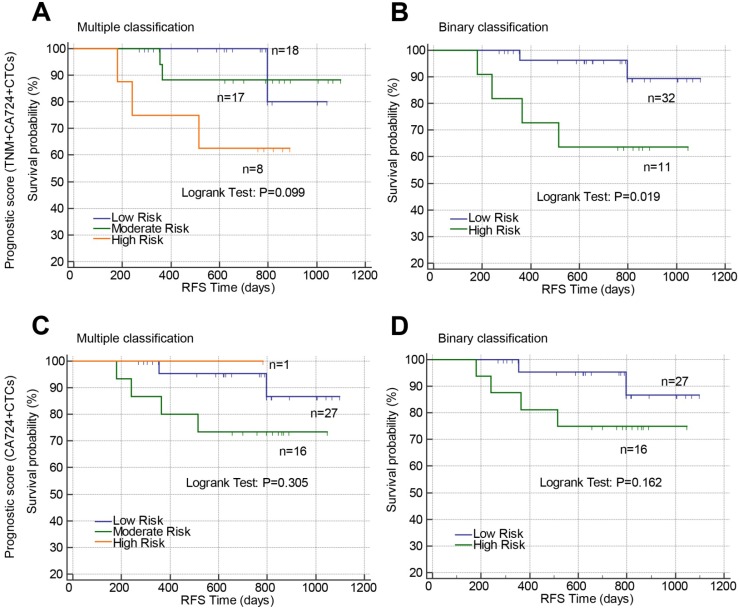
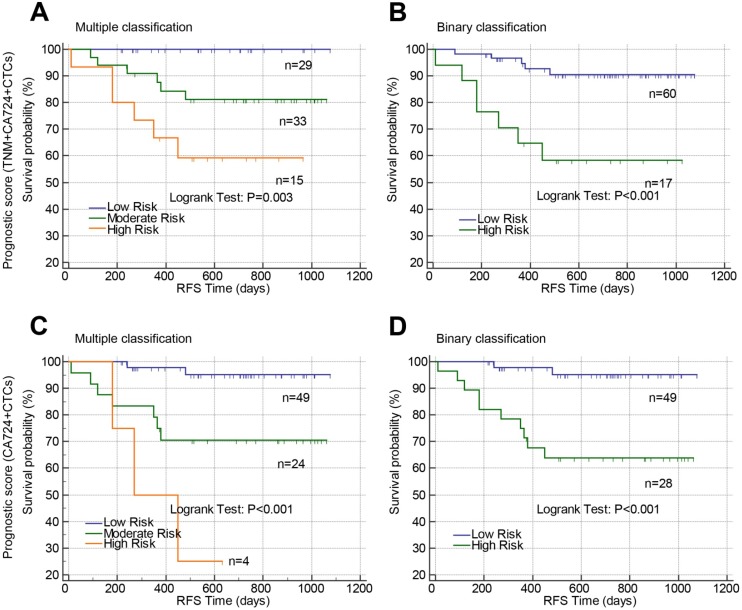
Background: It is urgent to develop robust prognostic biomarkers for non-metastatic colorectal cancer (CRC) patients undergoing surgery. The current study aimed to explore and compare the clinical significance of preoperative and postoperative blood tumor biomarkers including circulating tumor cells (CTCs), and develop prognostic models based on tumor biomarkers in patients with stage II-III CRC receiving surgery. Methods: A prospective study was performed to enroll 130 patients with stage II-III CRC receiving surgery between January 2015 and December 2017. Preoperative and postoperative blood tumor biomarkers including CTCs were detected and their prognostic value in predicting tumor recurrence-free survival (RFS) in stage II-III CRC were identified by Kaplan-Meier curves and Cox proportional hazard regression models. Results: CTCs counts within three postoperative days were significantly higher than preoperative CTCs (pre-CTCs). No significant association of pre-CTCs with clinical characteristics and tumor biomarkers was observed while positive postoperative CTCs (post-CTCs) were associated with female, older onset age, high TNM stage, tumor recurrence, and preoperative CEA. Kaplan-Meier curve with log-rank test and univariate Cox proportional hazard regression analysis suggested high N stage, TNM stage, positive pre-carbohydrate antigen (CA) 125, pre-CA19-9, post-CA125, post-CA19-9, post-CA72-4, post-carcinoembryonic antigen (CEA), and post-CTCs were correlated with poor RFS. In multivariate analysis, only TNM stage (adjusted HR=3.786, 95% CI=1.330-10.780; P=0.013), post-CA72-4 (adjusted HR=5.675, 95% CI=2.064-15.604; P=0.001), and post-CTCs (adjusted HR=2.739, 95% CI=1.042-7.200; P=0.041) were significantly correlated with poor RFS. We then developed prognostic models combining post-CTCs and post-CA72-4 with TNM stage or not to stratify the patients into different risk groups. These prognostic models exert a similar good performance in predicting tumor RFS in stage II-III CRC patients. Conclusions: Postoperative CTCs were prior to preoperative CTCs in predicting tumor recurrence survival in non-metastatic CRC patients undergoing surgery. We also developed CTCs-based prognostic models to predict tumor recurrence in stage II-III CRC, which might be used to identify the patients with high risk of recurrence and guide aggressive treatment to improve the clinical outcomes of those patients.
Keywords: circulating tumor cells; non-metastatic colorectal cancer; prognostic model; tumor recurrence survival.
Conflict of interest statement
Competing Interests: The authors have declared that no competing interest exists.
Figures

References
-
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68:394–424. - PubMed
-
- Edwards BK, Ward E, Kohler BA, Eheman C, Zauber AG, Anderson RN. et al. Annual report to the nation on the status of cancer, 1975-2006, featuring colorectal cancer trends and impact of interventions (risk factors, screening, and treatment) to reduce future rates. Cancer. 2010;116:544–73. - PMC - PubMed
-
- Fidler IJ. The pathogenesis of cancer metastasis: the 'seed and soil' hypothesis revisited. Nat Rev Cancer. 2003;3:453–8. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
