

Fascioliasis presenting as colon cancer liver metastasis on 18F-fluorodeoxyglucose positron emission tomography/computed tomography: A case report
- PMID: 31528248
- PMCID: PMC6717711
- DOI: 10.4254/wjh.v11.i8.656
Fascioliasis presenting as colon cancer liver metastasis on 18F-fluorodeoxyglucose positron emission tomography/computed tomography: A case report
Abstract
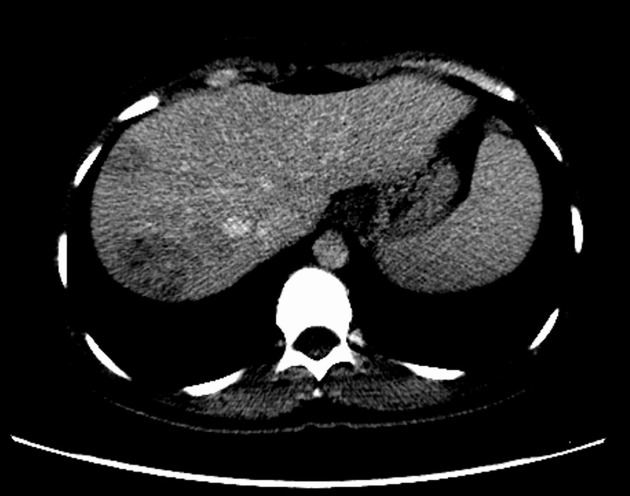
Background: Fascioliasis is caused by watercress and similar freshwater plants or drinking water or beverages contaminated with metacercariae. Fascioliasis can radiologically mimic many primary or metastatic liver tumors. Herein, we aimed to present the treatment process of a patient with fascioliasis mimicking colon cancer liver metastasis.
Case summary: A 35-year-old woman who underwent right hemicolectomy due to cecum cancer was referred to our clinic for management of colon cancer liver metastasis. Both computed tomography and 18F-fluorodeoxyglucose positron emission tomography revealed several tumoral lesions localized in the right lobe of the liver. After a 6-course FOLFOX (folinic acid, fluorouracil, oxaliplatin) and bevacizumab regimen, the hypermetabolic state on both liver and abdominal lymph nodes continued, and chemotherapy was extended to a 12-course regimen. The patient was referred to our institute when the liver lesions were detected to be larger on dynamic liver magnetic resonance imaging 6 weeks after completion of chemotherapy. Right hepatectomy was performed, and histopathological examination was compatible with fascioliasis. Fasciola hepatica IgG enzyme-linked immunosorbent assay was positive. The patient was administered two doses of triclabendazole (10 mg/kg/dose) 24 h apart. During the follow-up period, dilatation was detected in the common bile duct, and Fasciola parasites were extracted from the common bile duct by endoscopic retrograde cholangiopancreatography (ERCP). Triclabendazole was administered to the patient after ERCP.
Conclusion: Parasitic diseases, such as those caused by Fasciola hepatica, should be kept in mind in the differential diagnosis of primary or metastatic liver tumors, such as colorectal cancer liver metastasis, in patients living in endemic areas.
Keywords: Case report; Colon cancer liver metastasis; Fasciola hepatica; Misdiagnosis; Positron emission tomography.
Conflict of interest statement
Conflict-of-interest statement: The authors declare no conflicts of interest.
Figures





References
-
- Mas-Coma S, Bargues MD, Valero MA. Human fascioliasis infection sources, their diversity, incidence factors, analytical methods and prevention measures. Parasitology. 2018;145:1665–1699. - PubMed
-
- Lim JH, Mairiang E, Ahn GH. Biliary parasitic diseases including clonorchiasis, opisthorchiasis and fascioliasis. Abdom Imaging. 2008;33:157–165. - PubMed
-
- Teichmann D, Grobusch MP, Göbels K, Müller HP, Koehler W, Suttorp N. Acute fascioliasis with multiple liver abscesses. Scand J Infect Dis. 2000;32:558–560. - PubMed
-
- Aksoy DY, Kerimoğlu U, Oto A, Ergüven S, Arslan S, Unal S, Batman F, Bayraktar Y. Fasciola hepatica infection: clinical and computerized tomographic findings of ten patients. Turk J Gastroenterol. 2006;17:40–45. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
