

The case for a universal hepatitis C vaccine to achieve hepatitis C elimination
- PMID: 31530275
- PMCID: PMC6749704
- DOI: 10.1186/s12916-019-1411-9
The case for a universal hepatitis C vaccine to achieve hepatitis C elimination
Abstract
Background: The introduction of highly effective direct-acting antiviral (DAA) therapy for hepatitis C has led to calls to eliminate it as a public health threat through treatment-as-prevention. Recent studies suggest it is possible to develop a vaccine to prevent hepatitis C. Using a mathematical model, we examined the potential impact of a hepatitis C vaccine on the feasibility and cost of achieving the global WHO elimination target of an 80% reduction in incidence by 2030 in the era of DAA treatment.
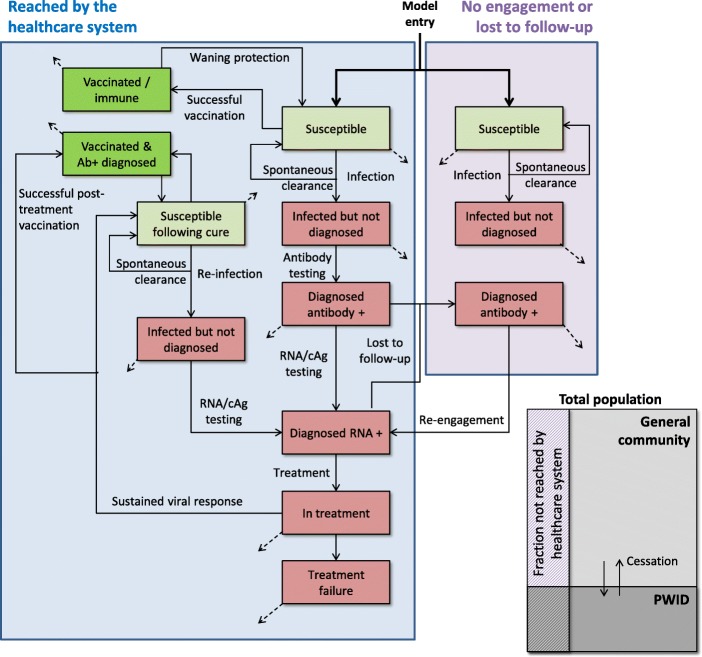
Methods: The model was calibrated to 167 countries and included two population groups (people who inject drugs (PWID) and the general community), features of the care cascade, and the coverage of health systems to deliver services. Projections were made for 2018-2030.
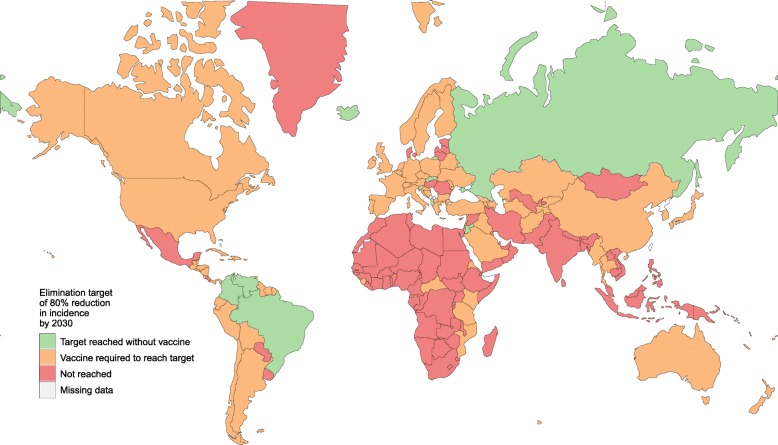
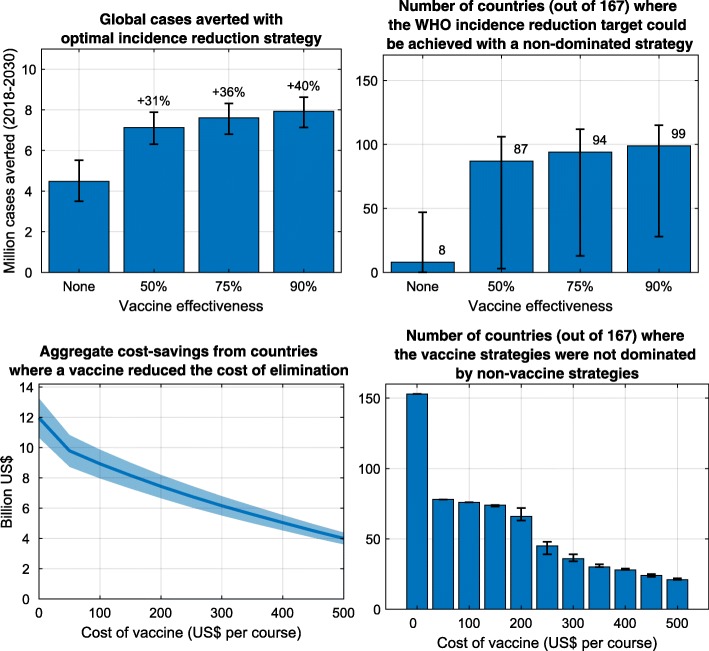
Results: The optimal incidence reduction strategy was to implement test and treat programmes among PWID, and in settings with high levels of community transmission undertake screening and treatment of the general population. With a vaccine available, the optimal strategy was to include vaccination within test and treat programmes, in addition to vaccinating adolescents in settings with high levels of community transmission. Of the 167 countries modelled, between 0 and 48 could achieve an 80% reduction in incidence without a vaccine. This increased to 15-113 countries if a 75% efficacious vaccine with a 10-year duration of protection were available. If a vaccination course cost US$200, vaccine use reduced the cost of elimination for 66 countries (40%) by an aggregate of US$7.4 (US$6.6-8.2) billion. For a US$50 per course vaccine, this increased to a US$9.8 (US$8.7-10.8) billion cost reduction across 78 countries (47%).
Conclusions: These findings strongly support the case for hepatitis C vaccine development as an urgent public health need, to ensure hepatitis C elimination is achievable and at substantially reduced costs for a majority of countries.
Keywords: Elimination; Hepatitis C; Mathematical model; Vaccine.
Conflict of interest statement
NS receives investigator-initiated research funding from Gilead Sciences unrelated to this work. AT is an advisory board member for Gilead Sciences, AbbVie, BMS, Merck, and Roche Diagnostics and a speaker for Gilead, Merck, BMS, AbbVie, and Roche Diagnostics. EB is developing vaccines as part of an Fp7 EU consortium (PEACHI) that includes GSK as a partner and has received funding to her institution from GSK to deliver studies in hepatitis C vaccines that encode class II invariant chain. MH and the Burnet Institute receive investigator-initiated research funding from Gilead Sciences, AbbVie, and BMS.
Figures

References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
