

Concordance Between Electronic Clinical Documentation and Physicians' Observed Behavior
- PMID: 31532513
- PMCID: PMC6751766
- DOI: 10.1001/jamanetworkopen.2019.11390
Concordance Between Electronic Clinical Documentation and Physicians' Observed Behavior
Abstract
Importance: Following the adoption of electronic health records into a regulatory environment designed for paper records, there has been little investigation into the accuracy of physician documentation.
Objective: To quantify the percentage of emergency physician documentation of the review of systems (ROS) and physical examination (PE) that observers can confirm.
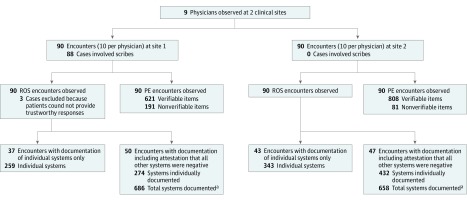
Design, setting, and participants: This case series took place at emergency departments in 2 academic medical centers between 2016 and 2018. Participants' patient encounters were observed to compare real-time performance with clinical documentation.
Exposures: Resident physicians were shadowed by trained observers for 20 encounters (10 encounters per physician per site) to obtain real-time observational data; associated electronic health record data were subsequently reviewed.
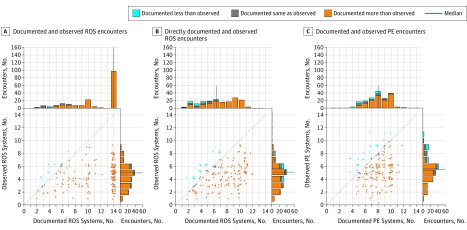
Main outcomes and measures: Number of confirmed ROS systems (range, 0-14) divided by the number of documented ROS systems (range, 0-14), and number of confirmed PE systems (range, 0-14) divided by the number of documented PE systems (range, 0-14).
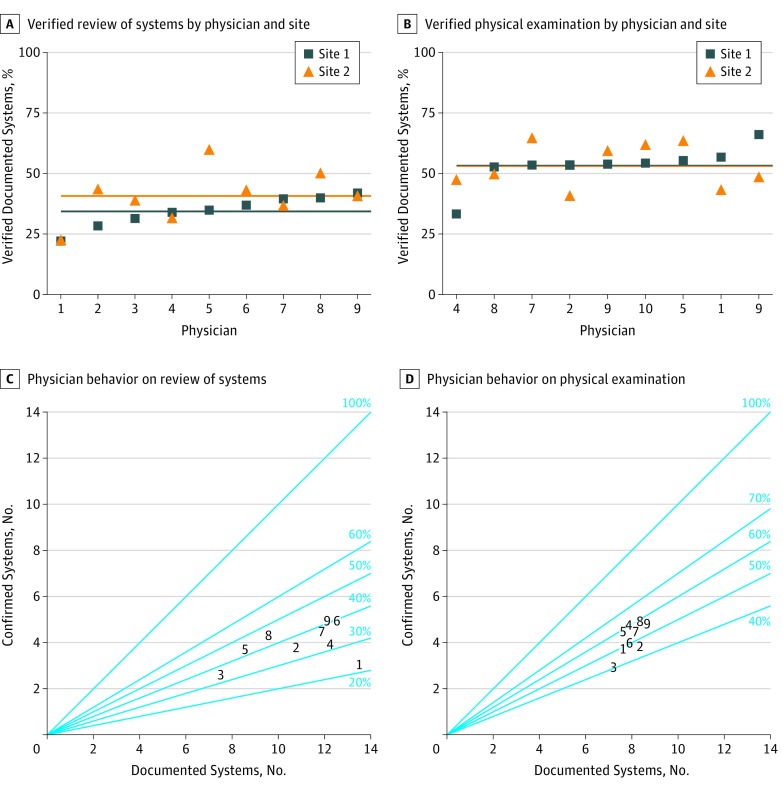
Results: The final study cohort included 9 licensed emergency medicine residents who evaluated a total of 180 patients (mean [SD] age, 48.7 [20.0] years; 91 [50.5%] women). For ROS, physicians documented a median (interquartile range [IQR]) of 14 (8-14) systems, while audio recordings confirmed a median (IQR) of 5 (3-6) systems. Overall, 755 of 1961 documented ROS systems (38.5%) were confirmed by audio recording data. For PE, resident physicians documented a median (IQR) of 8 (7-9) verifiable systems, while observers confirmed a median (IQR) of 5.5 (3-6) systems. Overall, 760 of 1429 verifiable documented PE systems (53.2%) were confirmed by concurrent observation. Interrater reliability for rating of ROS and PE was more than 90% for all measures.
Conclusions and relevance: In this study of 9 licensed year emergency medicine residents, there were inconsistencies between the documentation of ROS and PE findings in the electronic health record and observational reports. These findings raise the possibility that some documentation may not accurately represent physician actions. Further studies should be undertaken to determine whether this occurrence is widespread. However, because such studies are unlikely to be performed owing to institution-level barriers that exist nationwide, payers should consider removing financial incentives to generate lengthy documentation.
Conflict of interest statement
Figures
Comment in
-
Electronic Health Records-A System Only as Beneficial as Its Data.JAMA Netw Open. 2019 Sep 4;2(9):e1911679. doi: 10.1001/jamanetworkopen.2019.11679. JAMA Netw Open. 2019. PMID: 31532511 No abstract available.
References
-
- Centers for Medicare & Medicaid Services 1995 Documentation Guidelines for Evaluation and Management Services. https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN.... Accessed August 9, 2019.
-
- Centers for Medicare & Medicaid Services 1997 Documentation Guidelines for Evaluation and Management Services. https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN.... Accessed August 9, 2019.
-
- ECRI Institute Copy/paste: prevalence, problems, and best practices. https://www.ecri.org/Resources/HIT/CP_Toolkit/CopyPaste_Literature_final.... Accessed August 9, 2019.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
