

Prevalence of Screening for Food Insecurity, Housing Instability, Utility Needs, Transportation Needs, and Interpersonal Violence by US Physician Practices and Hospitals
- PMID: 31532515
- PMCID: PMC6752088
- DOI: 10.1001/jamanetworkopen.2019.11514
Prevalence of Screening for Food Insecurity, Housing Instability, Utility Needs, Transportation Needs, and Interpersonal Violence by US Physician Practices and Hospitals
Abstract
Importance: Social needs, including food, housing, utilities, transportation, and experience with interpersonal violence, are linked to health outcomes. Identifying patients with unmet social needs is a necessary first step to addressing these needs, yet little is known about the prevalence of screening.
Objective: To characterize screening for social needs by physician practices and hospitals.
Design, setting, and participants: Cross-sectional survey analyses of responses by physician practices and hospitals to the 2017-2018 National Survey of Healthcare Organizations and Systems. Responses were collected from survey participants from June 16, 2017, to August 17, 2018.
Exposures: Organizational characteristics, including participation in delivery and payment reform.
Main outcomes and measures: Self-report of screening patients for food insecurity, housing instability, utility needs, transportation needs, and experience with interpersonal violence.
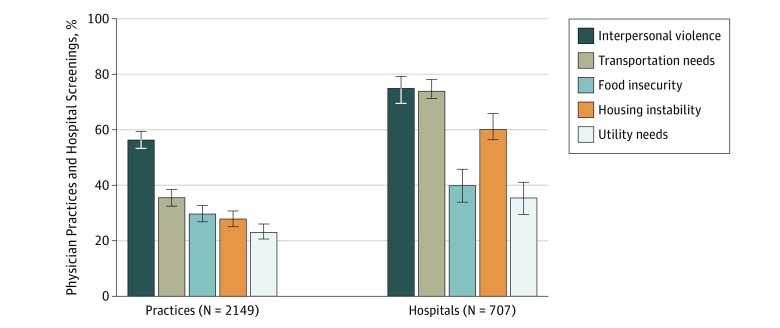
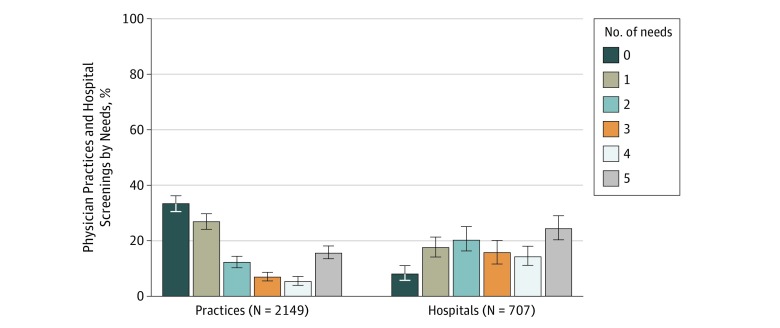
Results: Among 4976 physician practices, 2333 responded, a response rate of 46.9%. Among hospitals, 757 of 1628 (46.5%) responded. After eliminating responses because of ineligibility, 2190 physician practices and 739 hospitals remained. Screening for all 5 social needs was reported by 24.4% (95% CI, 20.0%-28.7%) of hospitals and 15.6% (95% CI, 13.4%-17.9%) of practices, whereas 33.3% (95% CI, 30.5%-36.2%) of practices and 8.0% (95% CI, 5.8%-11.0%) of hospitals reported no screening. Screening for interpersonal violence was most common (practices: 56.4%; 95% CI, 53.3%-2 59.4%; hospitals: 75.0%; 95% CI, 70.1%-79.3%), and screening for utility needs was least common (practices: 23.1%; 95% CI, 20.6%-26.0%; hospitals: 35.5%; 95% CI, 30.0%-41.0%) among both hospitals and practices. Among practices, federally qualified health centers (yes: 29.7%; 95% CI, 21.5%-37.8% vs no: 9.4%; 95% CI, 7.2%-11.6%; P < .001), bundled payment participants (yes: 21.4%; 95% CI, 17.1%-25.8% vs no: 10.7%; 95% CI, 7.9%-13.4%; P < .001), primary care improvement models (yes: 19.6%; 95% CI, 16.5%-22.6% vs no: 9.6%; 95% CI, 6.0%-13.1%; P < .001), and Medicaid accountable care organizations (yes: 21.8%; 95% CI, 17.4%-26.2% vs no: 11.2%; 95% CI, 8.6%-13.7%; P < .001) had higher rates of screening for all needs. Practices in Medicaid expansion states (yes: 17.7%; 95% CI, 14.8%-20.7% vs no: 11.4%; 95% CI, 8.1%-14.6%; P = .007) and those with more Medicaid revenue (highest tertile: 17.1%; 95% CI, 11.4%-22.7% vs lowest tertile: 9.0%; 95% CI, 6.1%-11.8%; P = .02) were more likely to screen. Academic medical centers were more likely than other hospitals to screen (49.5%; 95% CI, 34.6%-64.4% vs 23.0%; 95% CI, 18.5%-27.5%; P < .001).
Conclusions and relevance: This study's findings suggest that few US physician practices and hospitals screen patients for all 5 key social needs associated with health outcomes. Practices that serve disadvantaged patients report higher screening rates. The role of physicians and hospitals in meeting patients' social needs is likely to increase as more take on accountability for cost under payment reform. Physicians and hospitals may need additional resources to screen for or address patients' social needs.
Conflict of interest statement
Figures
Comment in
-
National Data on Social Risk Screening Underscore the Need for Implementation Research.JAMA Netw Open. 2019 Sep 4;2(9):e1911513. doi: 10.1001/jamanetworkopen.2019.11513. JAMA Netw Open. 2019. PMID: 31532510 Free PMC article. No abstract available.
References
-
- Castrucci B, Auerbach J. Meeting individual social needs falls short of addressing social determinants of health. Health Affairs Blog. https://www.healthaffairs.org/do/10.1377/hblog20190115.234942/full/. Published January 16, 2019. Accessed August 13, 2019. - DOI
-
- Solomon LS, Kanter MH. Health care steps up to social determinants of health: current context. Perm J. 2018;22:18-139. doi: 10.7812/TPP/18-139 - DOI
-
- Hostetter M, Klein S, McCarthy D Hennepin Health: a care delivery paradigm for new Medicaid beneficiaries. The Commonwealth Fund website. https://www.commonwealthfund.org/publications/case-study/2016/oct/hennep.... Published October 7, 2016. Accessed May 3, 2019.
