

Prediction of cardiovascular disease risk among people with severe mental illness: A cohort study
- PMID: 31532772
- PMCID: PMC6750572
- DOI: 10.1371/journal.pone.0221521
Prediction of cardiovascular disease risk among people with severe mental illness: A cohort study
Abstract
Objective: To determine whether contemporary sex-specific cardiovascular disease (CVD) risk prediction equations underestimate CVD risk in people with severe mental illness from the cohort in which the equations were derived.
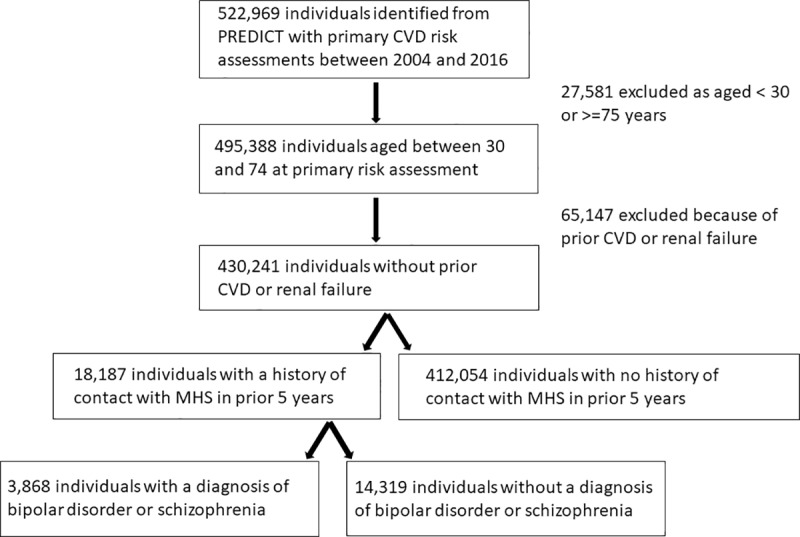
Methods: We identified people with severe mental illness using information on prior specialist mental health treatment. This group were identified from the PREDICT study, a prospective cohort study of 495,388 primary care patients aged 30 to 74 years without prior CVD that was recently used to derive new CVD risk prediction equations. CVD risk was calculated in participants with and without severe mental illness using the new equations and the predicted CVD risk was compared with observed risk in the two participant groups using survival methods.
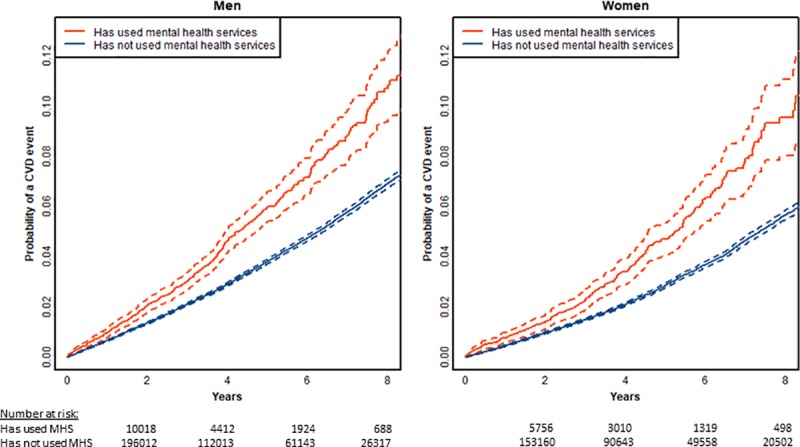
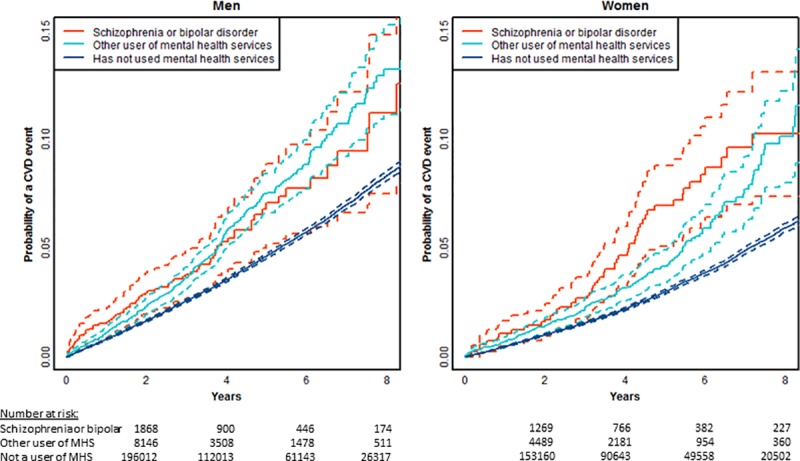
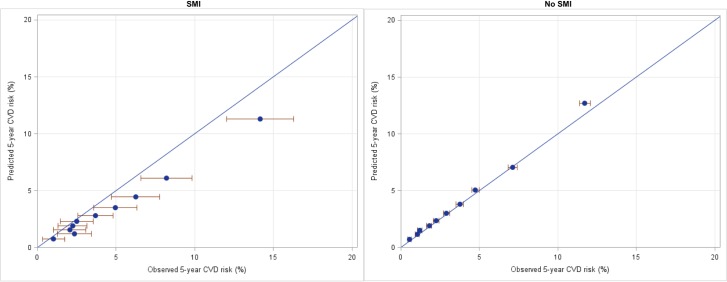
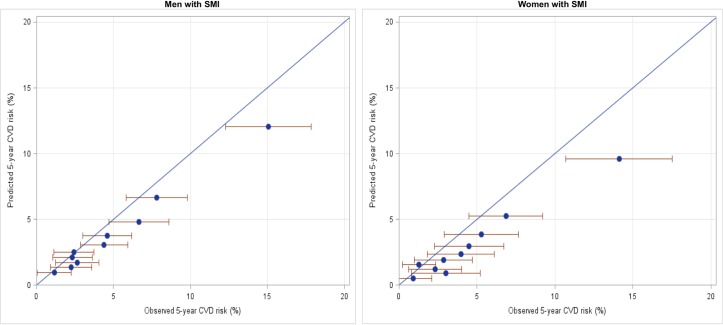
Results: 28,734 people with a history of recent contact with specialist mental health services, including those without a diagnosis of a psychotic disorder, were identified in the PREDICT cohort. They had a higher observed rate of CVD events compared to those without such a history. The PREDICT equations underestimated the risk for this group, with a mean observed:predicted risk ratio of 1.29 in men and 1.64 in women. In contrast the PREDICT algorithm performed well for those without mental illness.
Conclusions: Clinicians using CVD risk assessment tools that do not include severe mental illness as a predictor could by underestimating CVD risk by about one-third in men and two-thirds in women in this patient group. All CVD risk prediction equations should be updated to include mental illness indicators.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Correll CU, Solmi M, Veronese N, Bortolato B, Rosson S, Santonastaso P, et al. Prevalence, incidence and mortality from cardiovascular disease in patients with pooled and specific severe mental illness: a large-scale meta-analysis of 3,211,768 patients and 113,383,368 controls. World Psychiatry. 2017;16(2):163–80. 10.1002/wps.20420 - DOI - PMC - PubMed
-
- Cunningham R, Peterson D, Sarfati D, Stanley J, Collings S. Premature mortality in adults using New Zealand psychiatric services. New Zealand Medical Journal. 2014;127(1394). - PubMed
-
- Ruggeri M, Leese M, Thornicroft G, Bisoffi G, Tansella M. Definition and prevalence of severe and persistent mental illness. Br J Psychiatry. 2000;177(2):149–55. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
