

Temporal trends, predictors, and outcomes of acute kidney injury and hemodialysis use in acute myocardial infarction-related cardiogenic shock
- PMID: 31532793
- PMCID: PMC6750602
- DOI: 10.1371/journal.pone.0222894
Temporal trends, predictors, and outcomes of acute kidney injury and hemodialysis use in acute myocardial infarction-related cardiogenic shock
Abstract
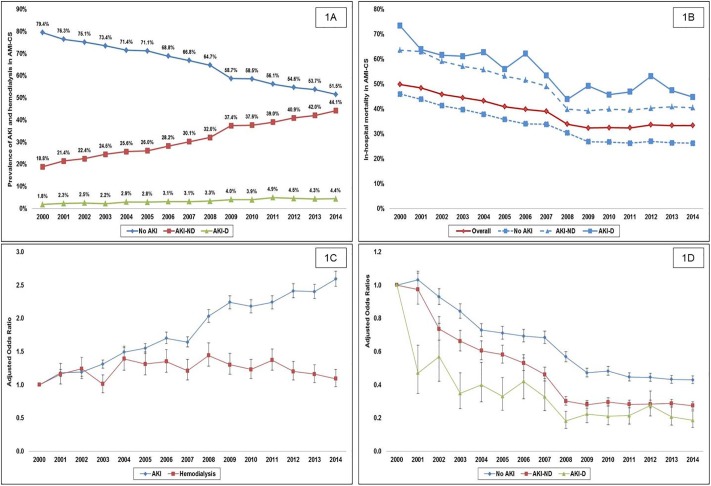
Background: There are limited data on acute kidney injury (AKI) complicating acute myocardial infarction with cardiogenic shock (AMI-CS). This study sought to evaluate 15-year national prevalence, temporal trends and outcomes of AKI with no need for hemodialysis (AKI-ND) and requiring hemodialysis (AKI-D) following AMI-CS.
Methods: This was a retrospective cohort study from 2000-2014 from the National Inpatient Sample (20% stratified sample of all community hospitals in the United States). Adult patients (>18 years) admitted with a primary diagnosis of AMI and secondary diagnosis of CS were included. The primary outcome was in-hospital mortality in cohorts with no AKI, AKI-ND, and AKI-D. Secondary outcomes included predictors, resource utilization and disposition.
Results: During this 15-year period, 440,257 admissions for AMI-CS were included, with AKI in 155,610 (35.3%) and hemodialysis use in 14,950 (3.4%). Older age, black race, non-private insurance, higher comorbidity, organ failure, and use of cardiac and non-cardiac organ support were associated with the AKI development and hemodialysis use. There was a 2.6-fold higher adjusted risk of developing AKI in 2014 compared to 2000. Presence of AKI-ND and AKI-D was associated with a 1.3 and 1.7-fold higher adjusted risk of mortality. Compared to the cohort without AKI, AKI-ND and AKI-D were associated with longer length of stay (9±10, 12±13, and 18±19 days respectively; p<0.001) and higher hospitalization costs ($101,859±116,204, $159,804±190,766, and $265,875 ± 254,919 respectively; p<0.001).
Conclusion: AKI-ND and AKI-D are associated with higher in-hospital mortality and resource utilization in AMI-CS.
Conflict of interest statement
Dr. Jaffe has been a consultant for Beckman, Abbott, Siemens, ET Healthcare, Sphing6toec, Quidel, and Novartis. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose. This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
References
-
- Vallabhajosyula S, Dunlay SM, Kashani K, Vallabhajosyula S, Vallabhajosyula S, Sundaragiri PR, et al. Temporal trends and outcomes of prolonged invasive mechanical ventilation and tracheostomy use in acute myocardial infarction with cardiogenic shock in the United States. Int J Cardiol. 2019;285:6–10. 10.1016/j.ijcard.2019.03.008 . - DOI - PubMed
-
- Vallabhajosyula S, Dunlay SM, Murphree DH, Barsness GW, Sandhu GS, Lerman A, et al. Cardiogenic shock in Takotsubo cardiomyopathy versus acute myocardial infarction: An 8-year national perspective on clinical characteristics, management, and outcomes. JACC Heart Fail. 2019; 7(6):469–476. 10.1016/j.jchf.2018.12.007 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
