

Polypill for Cardiovascular Disease Prevention in an Underserved Population
- PMID: 31532959
- PMCID: PMC6938029
- DOI: 10.1056/NEJMoa1815359
Polypill for Cardiovascular Disease Prevention in an Underserved Population
Abstract
Background: Persons with low socioeconomic status and nonwhite persons in the United States have high rates of cardiovascular disease. The use of combination pills (also called "polypills") containing low doses of medications with proven benefits for the prevention of cardiovascular disease may be beneficial in such persons. However, few data are available regarding the use of polypill therapy in underserved communities in the United States, in which adherence to guideline-based care is generally low.
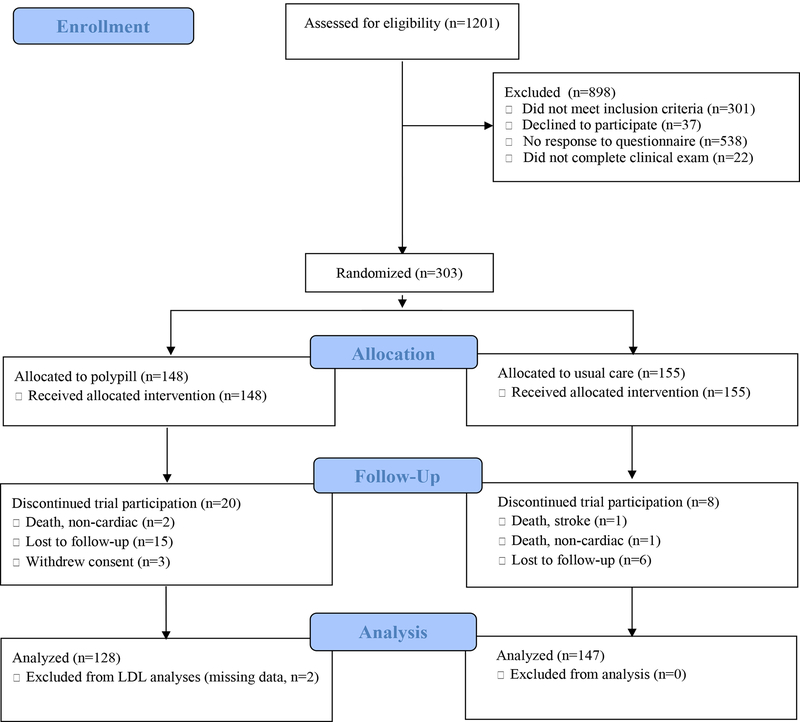
Methods: We conducted a randomized, controlled trial involving adults without cardiovascular disease. Participants were assigned to the polypill group or the usual-care group at a federally qualified community health center in Alabama. Components of the polypill were atorvastatin (at a dose of 10 mg), amlodipine (2.5 mg), losartan (25 mg), and hydrochlorothiazide (12.5 mg). The two primary outcomes were the changes from baseline in systolic blood pressure and low-density lipoprotein (LDL) cholesterol level at 12 months.
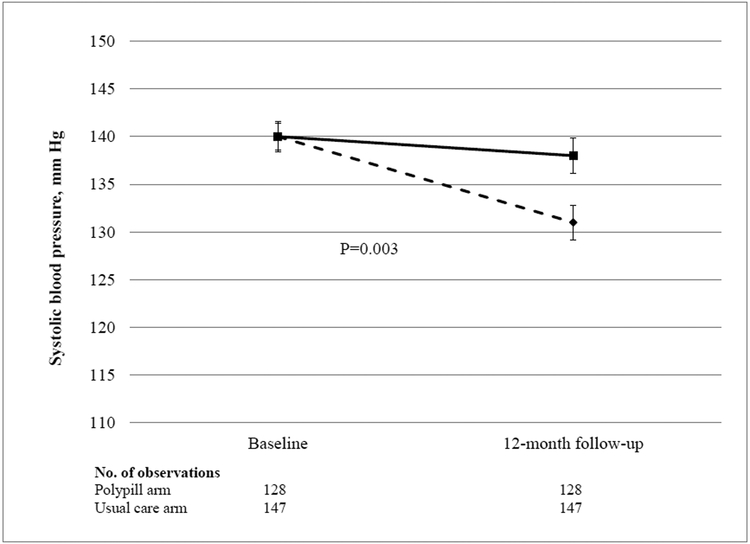
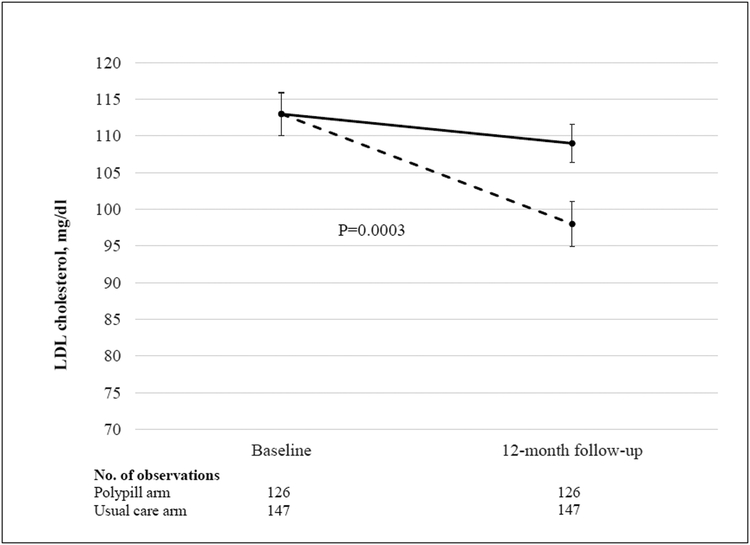
Results: The trial enrolled 303 adults, of whom 96% were black. Three quarters of the participants had an annual income below $15,000. The mean estimated 10-year cardiovascular risk was 12.7%, the baseline blood pressure was 140/83 mm Hg, and the baseline LDL cholesterol level was 113 mg per deciliter. The monthly cost of the polypill was $26. At 12 months, adherence to the polypill regimen, as assessed on the basis of pill counts, was 86%. The mean systolic blood pressure decreased by 9 mm Hg in the polypill group, as compared with 2 mm Hg in the usual-care group (difference, -7 mm Hg; 95% confidence interval [CI], -12 to -2; P = 0.003). The mean LDL cholesterol level decreased by 15 mg per deciliter in the polypill group, as compared with 4 mg per deciliter in the usual-care group (difference, -11 mg per deciliter; 95% CI, -18 to -5; P<0.001).
Conclusions: A polypill-based strategy led to greater reductions in systolic blood pressure and LDL cholesterol level than were observed with usual care in a socioeconomically vulnerable minority population. (Funded by the American Heart Association Strategically Focused Prevention Research Network and the National Institutes of Health; ClinicalTrials.gov number, NCT02278471.).
Copyright © 2019 Massachusetts Medical Society.
Figures
Comment in
-
Benefit of polypills in a low socioeconomic community in the USA.Nat Rev Cardiol. 2019 Dec;16(12):701. doi: 10.1038/s41569-019-0295-x. Nat Rev Cardiol. 2019. PMID: 31578517 No abstract available.
-
Polypill for Cardiovascular Disease Prevention in an Underserved Population.N Engl J Med. 2020 Jan 2;382(1):94. doi: 10.1056/NEJMc1914047. N Engl J Med. 2020. PMID: 31875509 No abstract available.
-
Polypill for Cardiovascular Disease Prevention in an Underserved Population.N Engl J Med. 2020 Jan 2;382(1):94-95. doi: 10.1056/NEJMc1914047. N Engl J Med. 2020. PMID: 31875510 Free PMC article. No abstract available.
References
-
- Whelton PK, Carey RM, Aronow WS, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol 2018;71:e127–e248. - PubMed
-
- Hajjar I, Kotchen TA. Trends in prevalence, awareness, treatment, and control of hypertension in the United States, 1988–2000. JAMA 2003;290:199–206. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical