

The Transitional Heart: From Early Embryonic and Fetal Development to Neonatal Life
- PMID: 31533099
- PMCID: PMC7265763
- DOI: 10.1159/000501906
The Transitional Heart: From Early Embryonic and Fetal Development to Neonatal Life
Abstract
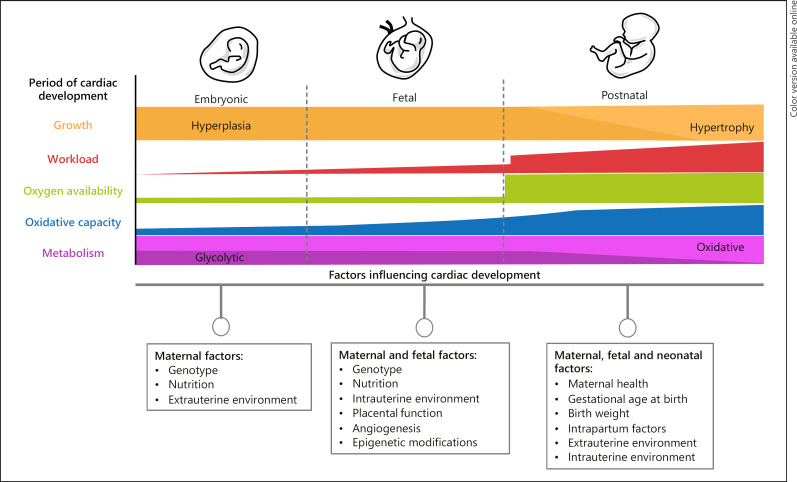
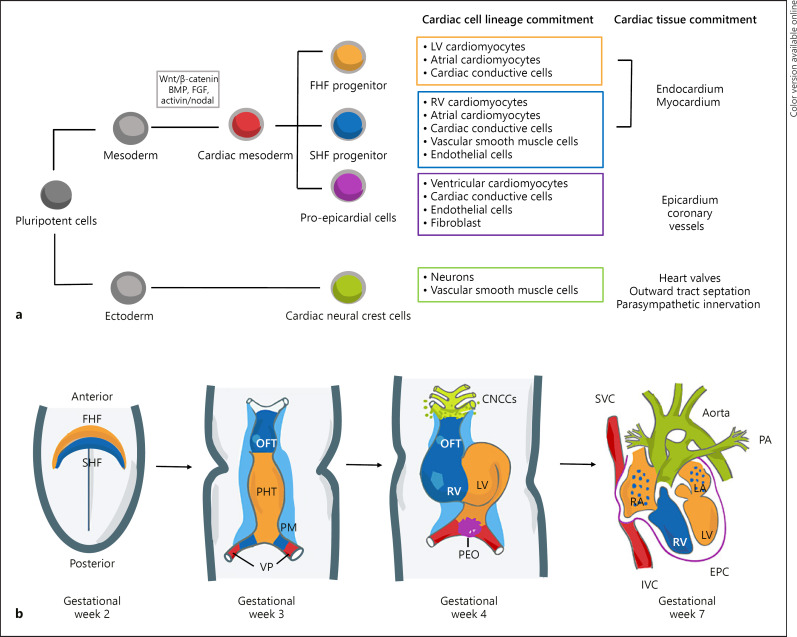
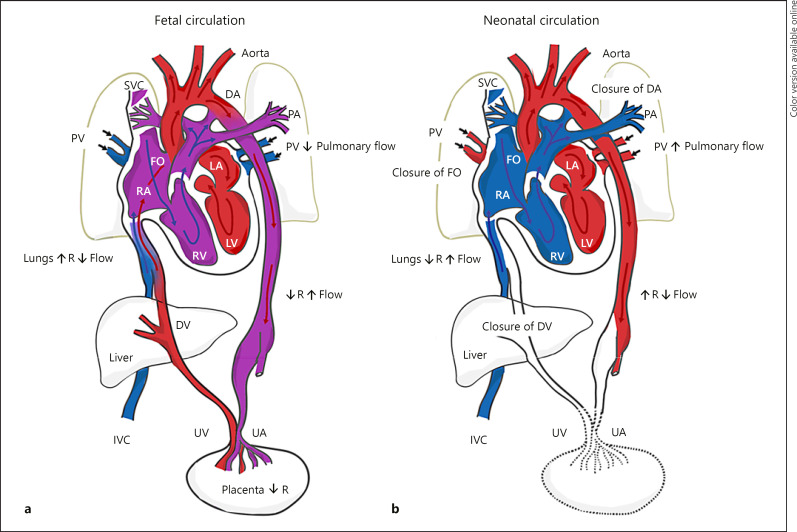
Formation of the human heart involves complex biological signals, interactions, specification of myocardial progenitor cells, and heart tube looping. To facilitate survival in the hypoxemic intrauterine environment, the fetus possesses structural, physiological, and functional cardiovascular adaptations that are fundamentally different from the neonate. At birth, upon separation from the placental circulation, the neonatal cardiovascular system takes over responsibility of vital processes for survival. The transition from the fetal to neonatal circulation is considered to be a period of intricate physiological, anatomical, and biochemical changes in the cardiovascular system. With a successful cardiopulmonary transition to the extrauterine environment, the fetal shunts are functionally modified or eliminated, enabling independent life. Investigations using medical imaging tools such as ultrasound and magnetic resonance imaging have helped to define normal and abnormal patterns of cardiac remodeling both in utero and ex utero. This has not only allowed for a better understanding of how congenital cardiac malformations alter the hemodynamic transition to the extrauterine environment but also how other more common complications during pregnancy including intrauterine growth restriction, preeclampsia, and preterm delivery adversely affect offspring cardiac remodeling during this early transitional period. This review article describes key cardiac progenitors involved in embryonic heart development; the cellular, physiological, and anatomical changes during the transition from fetal to neonatal circulation; as well as the unique impact that different pregnancy complications have on cardiac remodeling.
Keywords: Cardiac development; Developmental biology; Fetal heart; Neonatal heart; Transitional physiology.
© 2019 The Author(s) Published by S. Karger AG, Basel.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Bulatovic I, Månsson-Broberg A, Sylvén C, Grinnemo KH. Human fetal cardiac progenitors: the role of stem cells and progenitors in the fetal and adult heart. Best Pract Res Clin Obstet Gynaecol. 2016 Feb;31:58–68. - PubMed
-
- Buckingham M, Meilhac S, Zaffran S. Building the mammalian heart from two sources of myocardial cells. Nat Rev Genet. 2005 Nov;6((11)):826–35. - PubMed
-
- Finnemore A, Groves A. Physiology of the fetal and transitional circulation. Semin Fetal Neonatal Med. 2015 Aug;20((4)):210–6. - PubMed
-
- Berhrsin J, Gibson A. Cardiovascular system adaptation at birth. Paediatr Child Health. 2011;21((1)):1–6.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
