

Gallstone Ileus: Management and Clinical Outcomes
- PMID: 31533295
- PMCID: PMC6780297
- DOI: 10.3390/medicina55090598
Gallstone Ileus: Management and Clinical Outcomes
Abstract
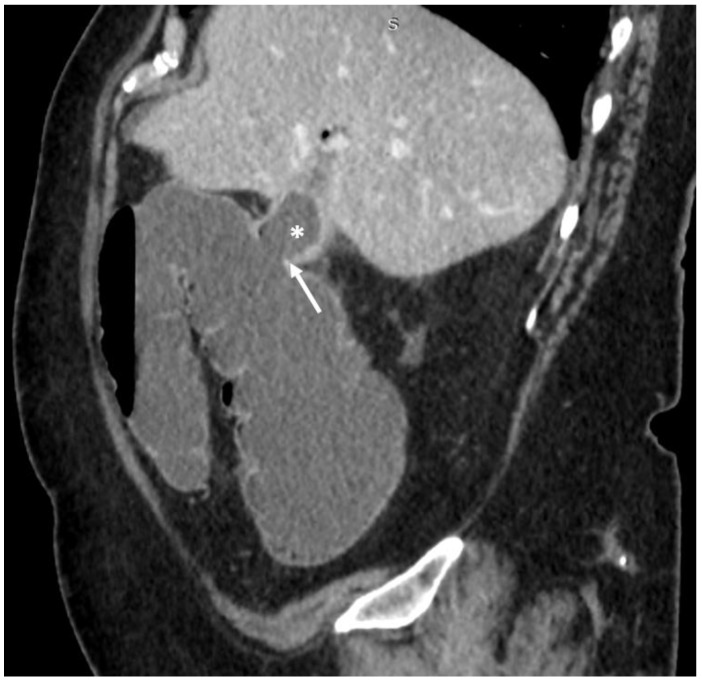
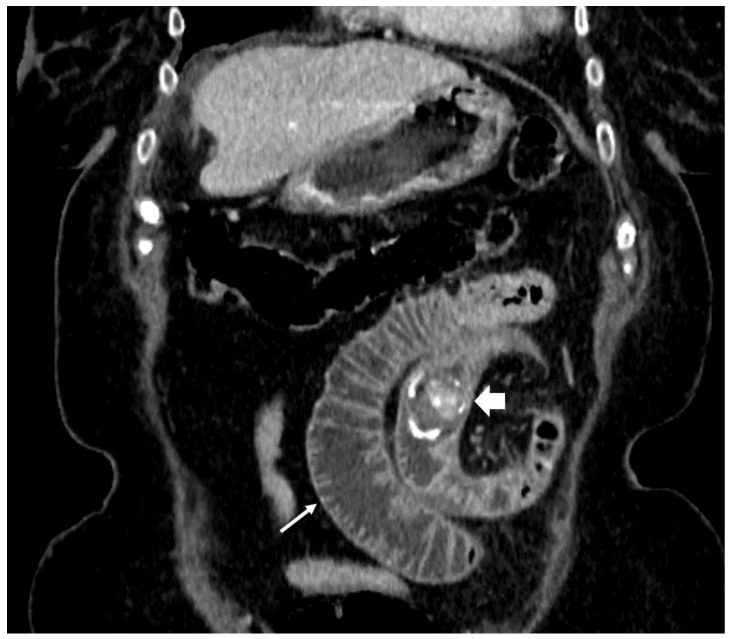
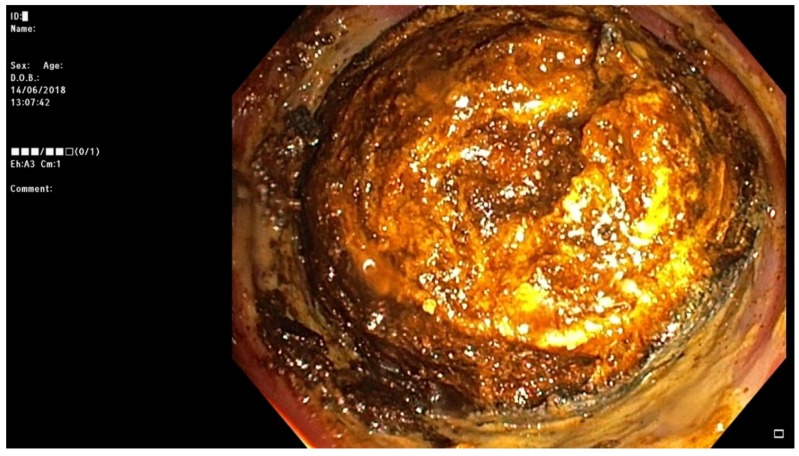
Background: Gallstone or biliary ileus is a late complication of gallstone disease. It accounts for 1%-4% of all bowel obstructions and is more common in elderly patients. The preferred treatment option is to mechanically remove the impacted stones. It is done surgically using open or laparoscopic approach and rarely, when stones are impacted in the colon, endoscopically. In this paper we present five consecutive cases of gallstone ileus and describe possible diagnostic and minimally invasive treatment options. Case presentation: During a five-month period a total of five patients were treated for gallstone ileus. All patients were female and from 48 to 87 years of age. Symptoms were not specific and common for all small bowel obstructions. Upon admission the patients also had unspecific laboratory findings-neutrophilic leukocytosis and various C-reactive protein concentrations, ranging from 8 to 347 mg/L. According to the hospital protocol, all patients initially underwent an abdominal ultrasound, which was inconclusive, and therefore every patient additionally had a CT scan with intravenous contrast. After these two diagnostic modalities one patient still did not have the definitive gallstone ileus diagnosis, as the ectopic stone was not visible. Four patients in our case series were treated using minimally invasive methods: in one case the stone was removed endoscopically, and laparoscopically in the other three. Treatment outcomes were good in four cases as the patients fully recovered, however one patient suffered a massive cerebral infarction after the operation and passed away. Conclusions: Gallstone ileus is a rare and difficult-to-diagnose condition. Management of these patients in every case should be individualized, as there are many options, each with their own advantages and disadvantages. We show that minimally invasive treatment such as colonoscopy or laparoscopy is possible in these cases.
Keywords: biliary ileus; diagnosis; endoscopy; gallstone; laparoscopy; treatment.
Conflict of interest statement
The authors declare no conflict of interest.
Figures





References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
