

Creatine as a Candidate to Prevent Statin Myopathy
- PMID: 31533334
- PMCID: PMC6770148
- DOI: 10.3390/biom9090496
Creatine as a Candidate to Prevent Statin Myopathy
Abstract
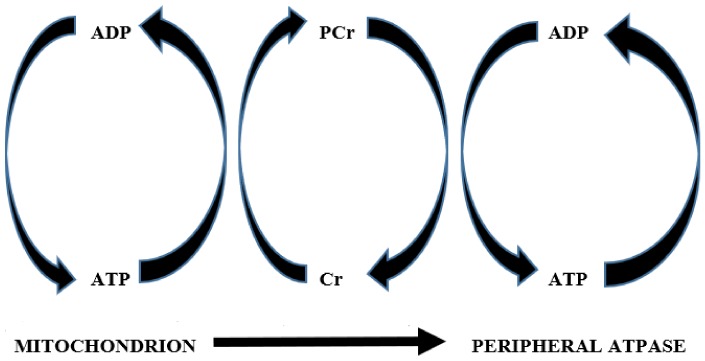
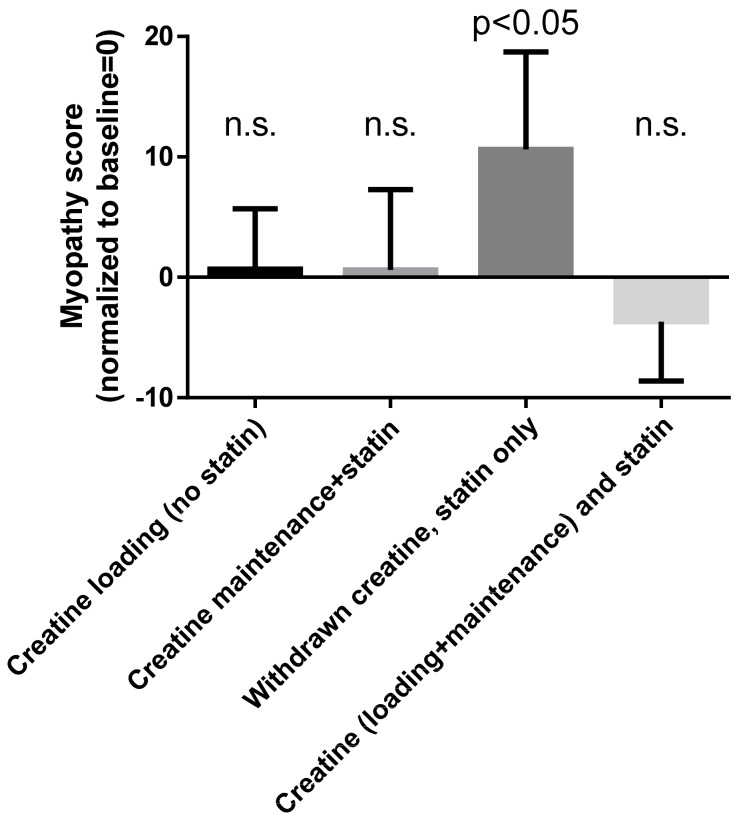
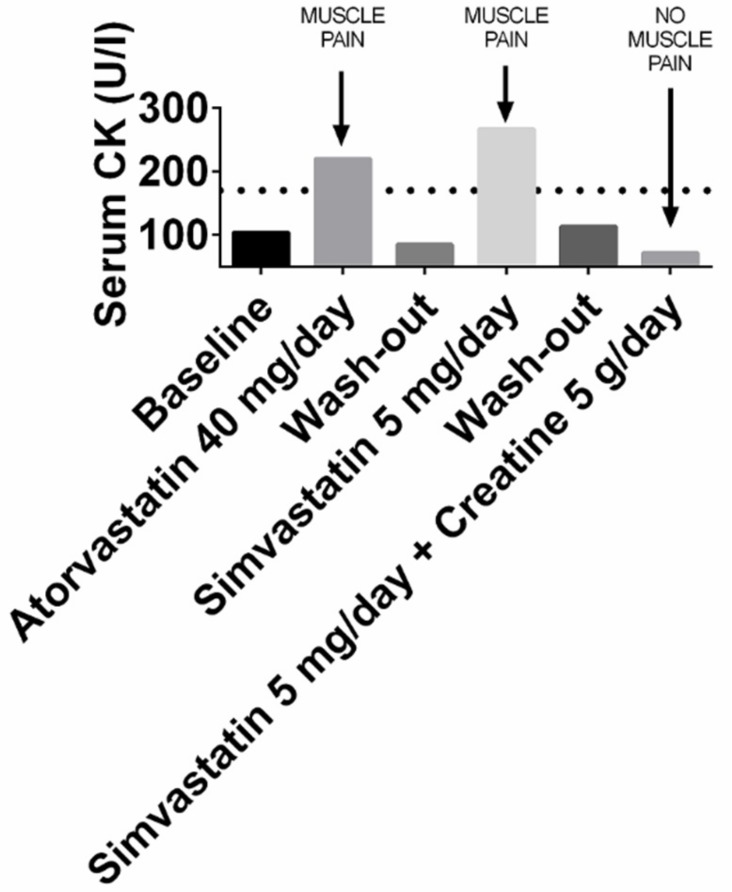
Statins prevent cardiovascular diseases, yet their use is limited by the muscle disturbances they cause. Rarely, statin-induced myopathy is autoimmune, but more commonly it is due to direct muscle toxicity. Available evidence suggests that statin-induced creatine deficiency might be a major cause of this toxicity, and that creatine supplementation prevents it. Statins inhibit guanidinoacetate methyl transferase (GAMT), the last enzyme in the synthesis of creatine; thus, they decrease its intracellular content. Such decreased content could cause mitochondrial impairment, since creatine is the final acceptor of the phosphate group of adenosine triphosphate (ATP) at the end of mitochondrial oxidative phosphorylation. Decreased cellular synthesis of ATP would follow. Accordingly, ATP synthesis is decreased in statin-treated cells. In vitro, creatine supplementation prevents the opening of the mitochondrial permeability transition pore that is caused by statins. Clinically, creatine administration prevents statin myopathy in statin-intolerant patients. Additional research is warranted to hopefully confirm these findings. However, creatine is widely used by athletes with no adverse events, and has demonstrated to be safe even in double-blind, placebo-controlled trials of elderly individuals. Thus, it should be trialed, under medical supervision, in patients who cannot assume statin due to the occurrence of muscular symptoms.
Keywords: creatine; mitochondria; muscle; myalgia; myopathy; pathogenesis; pathophysiology; prevention; statin; treatment.
Conflict of interest statement
Both authors are founding members of NovaNeuro Srl, an academic spinoff that ideates, produces and commercializes dietary supplements based on creatine.
Figures
Similar articles
-
Creatine, guanidinoacetate and homoarginine in statin-induced myopathy.Amino Acids. 2020 Jul;52(6-7):1067-1069. doi: 10.1007/s00726-020-02865-w. Epub 2020 Jun 27. Amino Acids. 2020. PMID: 32594255 Free PMC article.
-
The role of mitochondria in statin-induced myopathy.Eur J Clin Invest. 2015 Jul;45(7):745-54. doi: 10.1111/eci.12461. Epub 2015 Jun 15. Eur J Clin Invest. 2015. PMID: 25991405 Review.
-
Presence of guanidinoacetate may compensate creatine absence and account for less statin-induced muscle damage in GAMT-deficient compared to AGAT-deficient mice.Amino Acids. 2020 Apr;52(4):667-669. doi: 10.1007/s00726-020-02838-z. Epub 2020 Mar 14. Amino Acids. 2020. PMID: 32172372 No abstract available.
-
Mechanisms of statin-associated skeletal muscle-associated symptoms.Pharmacol Res. 2020 Apr;154:104201. doi: 10.1016/j.phrs.2019.03.010. Epub 2019 Mar 12. Pharmacol Res. 2020. PMID: 30877064 Review.
-
Statin-associated autoimmune myopathy and anti-HMGCR autoantibodies.Muscle Nerve. 2013 Oct;48(4):477-83. doi: 10.1002/mus.23854. Epub 2013 Aug 30. Muscle Nerve. 2013. PMID: 23519993 Review.
Cited by
-
Intersection between Obesity, Dietary Selenium, and Statin Therapy in Brazil.Nutrients. 2021 Jun 12;13(6):2027. doi: 10.3390/nu13062027. Nutrients. 2021. PMID: 34204631 Free PMC article. Review.
-
Chronic Dialysis Patients Are Depleted of Creatine: Review and Rationale for Intradialytic Creatine Supplementation.Nutrients. 2021 Aug 6;13(8):2709. doi: 10.3390/nu13082709. Nutrients. 2021. PMID: 34444869 Free PMC article.
-
Low-Dose Creatine Supplementation May Be Effective in Early-Stage Statin Myopathy: A Preliminary Study.J Clin Med. 2024 Nov 27;13(23):7194. doi: 10.3390/jcm13237194. J Clin Med. 2024. PMID: 39685653 Free PMC article.
-
Systematic Investigations on the Metabolic and Transcriptomic Regulation of Lactate in the Human Colon Epithelial Cells.Int J Mol Sci. 2022 Jun 2;23(11):6262. doi: 10.3390/ijms23116262. Int J Mol Sci. 2022. PMID: 35682941 Free PMC article.
-
Statins Neuromuscular Adverse Effects.Int J Mol Sci. 2022 Jul 28;23(15):8364. doi: 10.3390/ijms23158364. Int J Mol Sci. 2022. PMID: 35955495 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
