

The effect of smoke-free legislation on the mortality rate of acute myocardial infarction: a meta-analysis
- PMID: 31533693
- PMCID: PMC6749716
- DOI: 10.1186/s12889-019-7408-7
The effect of smoke-free legislation on the mortality rate of acute myocardial infarction: a meta-analysis
Abstract
Background: Several studies have demonstrated that smoke-free legislation is associated with a reduced risk of mortality from acute myocardial infarction (AMI). This study aimed to examine and quantify the potential effect of smoke-free legislation on AMI mortality rate in different countries.
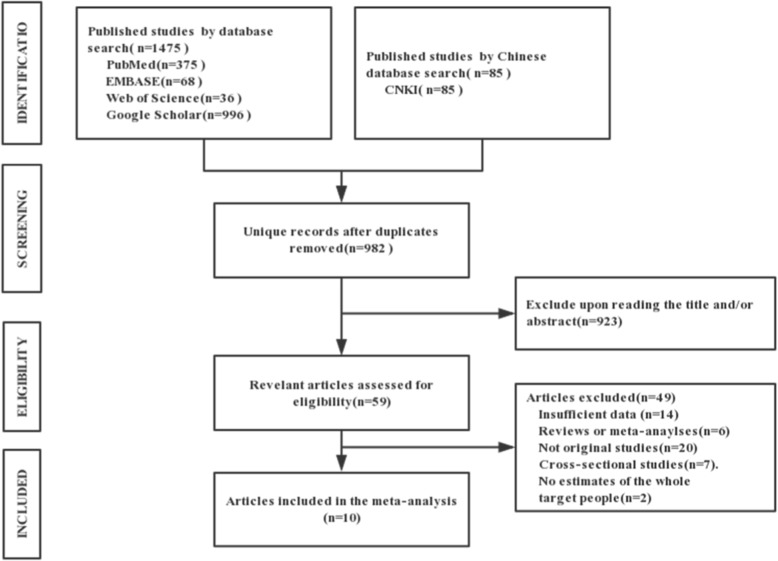
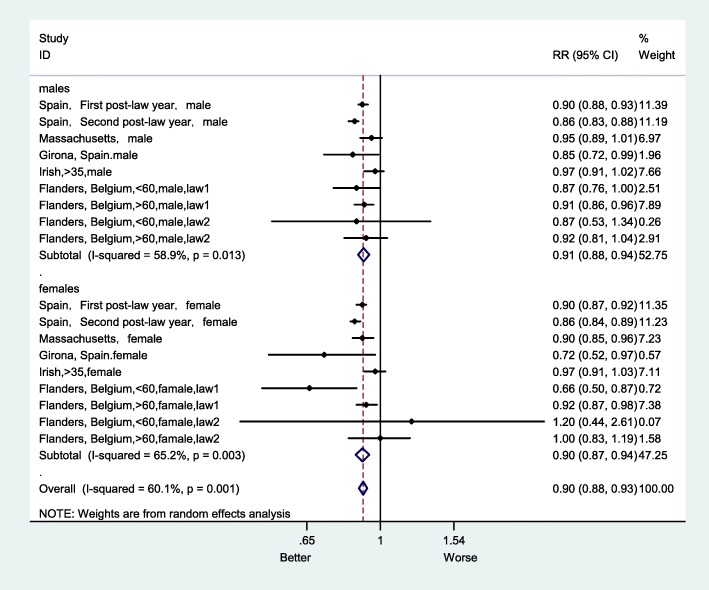
Methods: Studies were identified using a systematic search of the scientific literature from electronic databases, including PubMed, Web of Science, ScienceDirect, Embase, Google Scholar, and China National Knowledge Infrastructure (CNKI), from their inception through September 30, 2017. A random effects model was employed to estimate the overall effects of smoke-free legislation on the AMI mortality rate. Subgroup analysis was performed to explore the possible causes of heterogeneity in risk estimates based on sex and age. The results of meta-analysis after excluding the studies with a high risk of bias were reported in this study.
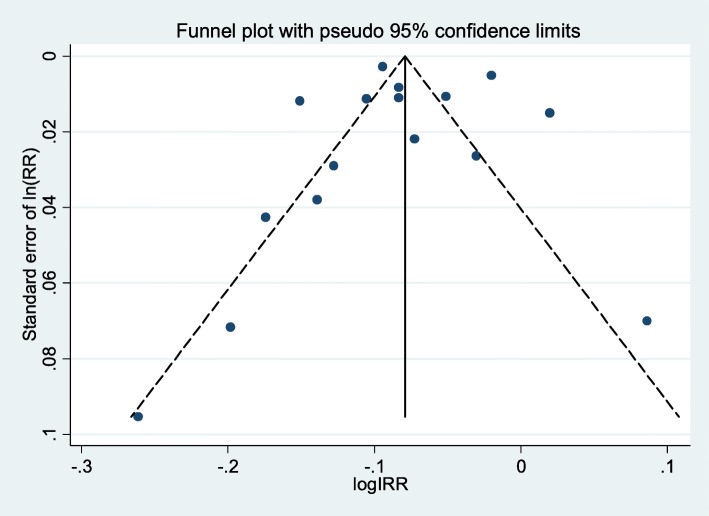
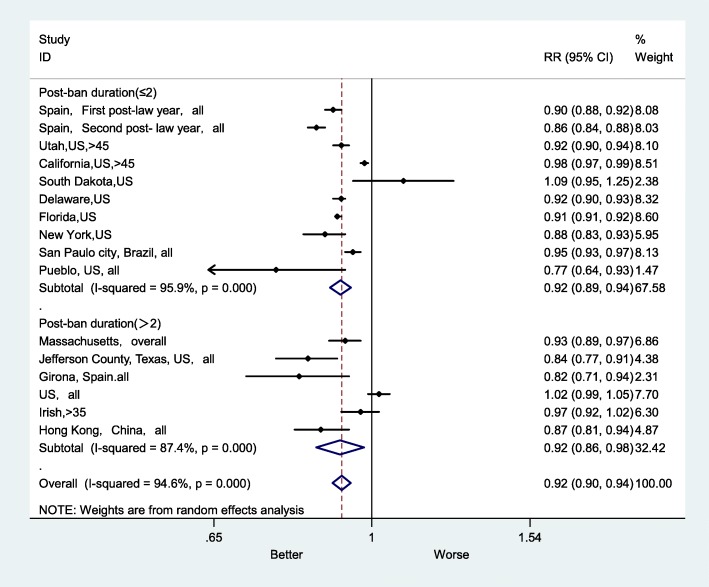
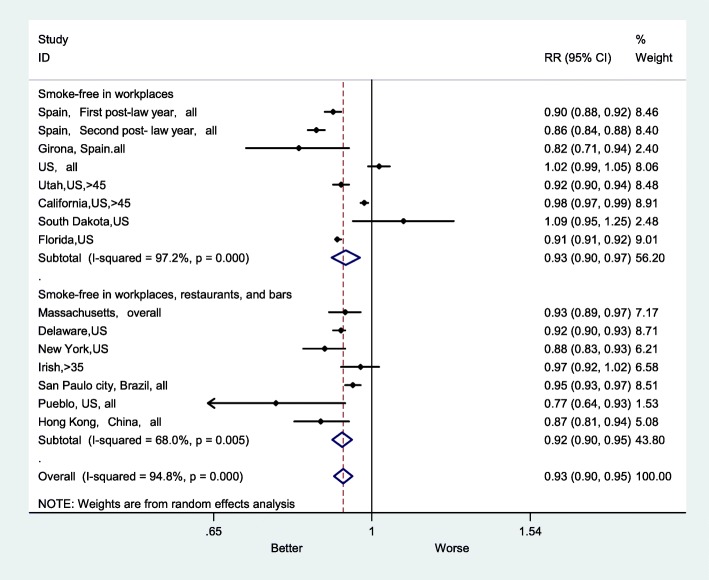
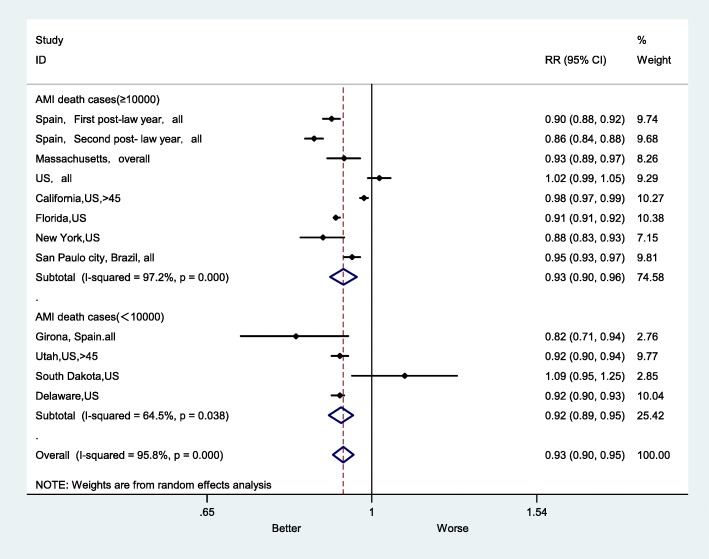
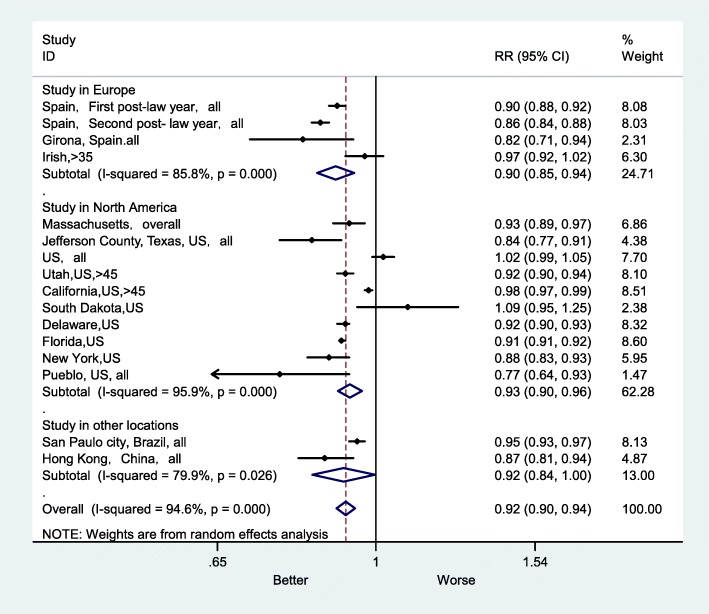
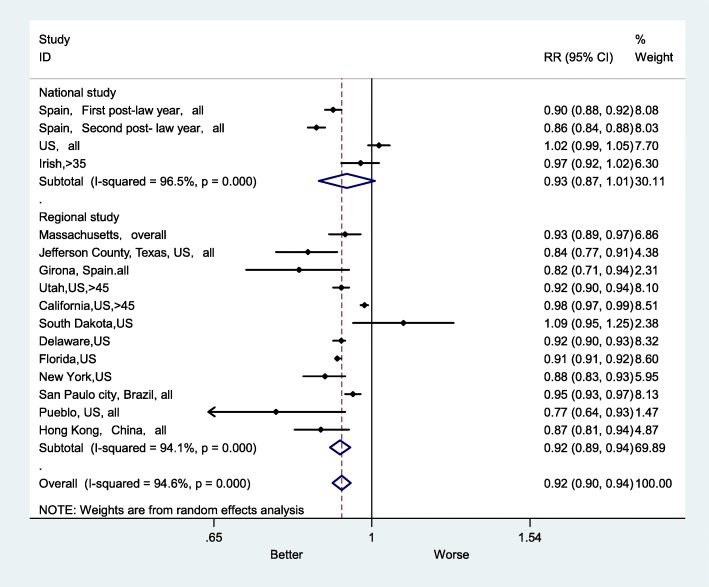
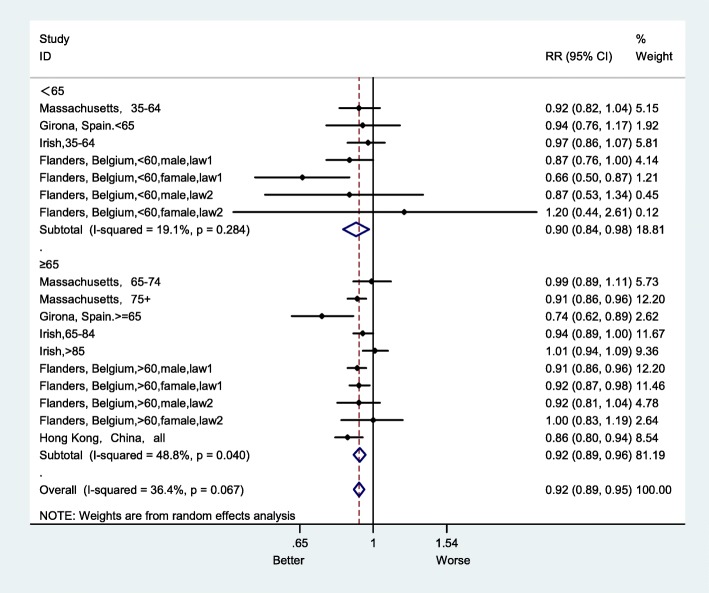
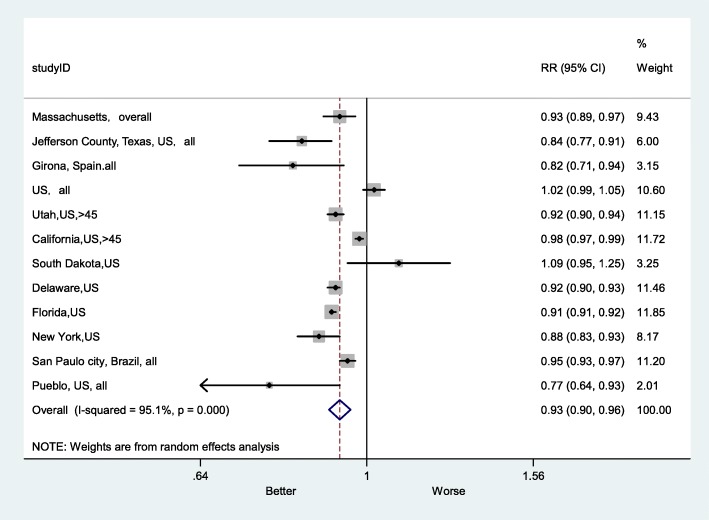
Results: A total of 10 eligible studies with 16 estimates of effect size were included in this meta-analysis. Significant heterogeneity in the risk estimates was identified (overall I2 = 94.6%, p < 0.001). Therefore, a random effects model was utilized to estimate the overall effect of smoke-free legislation. There was an 8% decline in AMI mortality after introducing smoke-free legislation (RR = 0.92, 95% confidence interval (CI): 0.90-0.94). The results of subgroup analyses showed that smoke-free legislation was significantly associated with lower rates of mortality for the following 5 diagnostic subgroups: smoke-free in workplaces, restaurants and bars (RR = 0.92, 95% CI: 0.90-0.95), smaller sample size (RR = 0.92, 95% CI: 0.89-0.95), study location in Europe (RR = 0.90, 95% CI: 0.85-0.94), regional study area (RR = 0.92, 95% CI: 0.89-0.94), and no previous local smoke-free legislation (RR = 0.91, 95% CI: 0.90-0.93). However, there was not much difference in AMI mortality rates after the legislation between the longer (RR = 0.92, 95% CI: 0.86-0.98) and shorter follow-up duration subgroups (RR = 0.92, 95% CI: 0.89-0.94).
Conclusion: Smoke-free legislation could significantly reduce the AMI mortality rate by 8%. The reduction in the AMI mortality rate was more significant in studies with more comprehensive laws, without prior smoke-free bans, with a smaller sample size, at the regional level, and with a location in Europe.
Keywords: Acute myocardial infarction (AMI); Meta-analysis; Smoke-free legislation; Systematic review.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
-
- Organization WH: WHO report on the global tobacco epidemic, 2013. Enforcing bans on tobacco advertising, promotion and sponsorship 2013.
-
- Reitsma MB, Fullman N, Ng M, Salama JS, Abajobir A, Abate KH, Abbafati C, Abera SF, Abraham B, Abyu GY. Smoking prevalence and attributable disease burden in 195 countries and territories, 1990–2015: a systematic analysis from the Global Burden of Disease Study 2015. Lancet. 2017;389(10082):1885–1906. - PMC - PubMed
-
- Barnoya J, Glantz SA. Cardiovascular effects of secondhand smoke: nearly as large as smoking. Circulation. 2005;111(20):2684–2698. - PubMed
-
- Öberg M, Jaakkola MS, Woodward A, Peruga A, Prüss-Ustün A. Worldwide burden of disease from exposure to second-hand smoke: a retrospective analysis of data from 192 countries. Lancet. 2011;377(9760):139–146. - PubMed
-
- U.S. Department of Health and Human Services : How tobacco smoke causes disease: The biology and behavioral basis for smoking-attributable disease: A report of the surgeon general. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health, 2010. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
