

Advances in β-cell replacement therapy for the treatment of type 1 diabetes
- PMID: 31533905
- PMCID: PMC6951435
- DOI: 10.1016/S0140-6736(19)31334-0
Advances in β-cell replacement therapy for the treatment of type 1 diabetes
Abstract
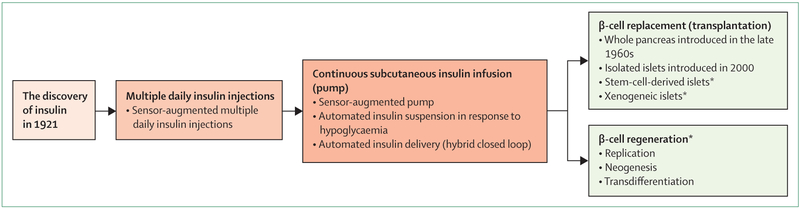
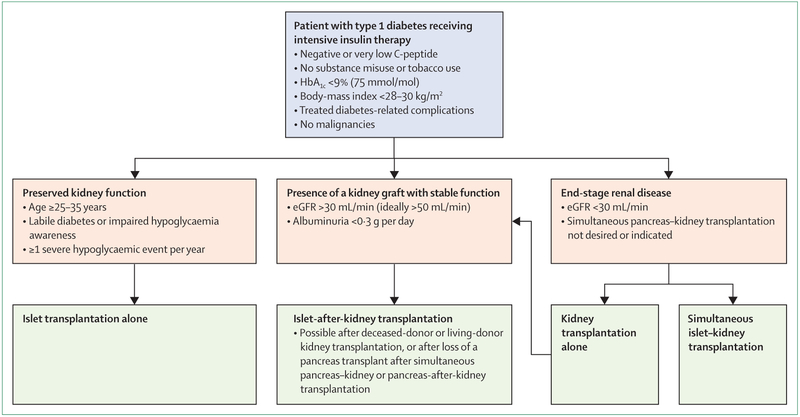
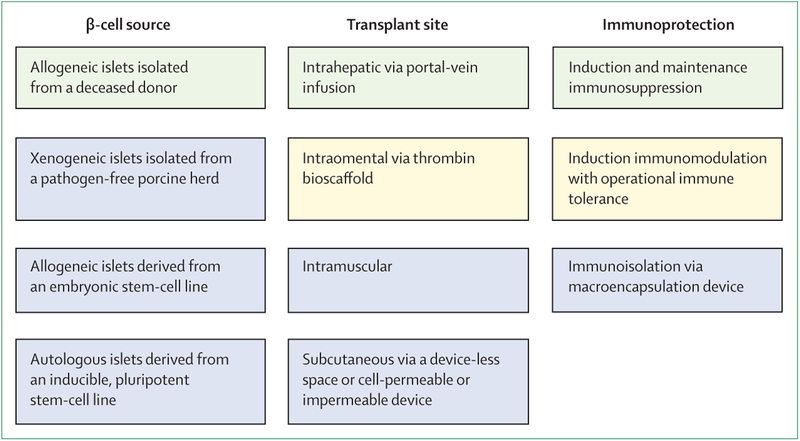
The main goal of treatment for type 1 diabetes is to control glycaemia with insulin therapy to reduce disease complications. For some patients, technological approaches to insulin delivery are inadequate, and allogeneic islet transplantation is a safe alternative for those patients who have had severe hypoglycaemia complicated by impaired hypoglycaemia awareness or glycaemic lability, or who already receive immunosuppressive drugs for a kidney transplant. Since 2000, intrahepatic islet transplantation has proven efficacious in alleviating the burden of labile diabetes and preventing complications related to diabetes, whether or not a previous kidney transplant is present. Age, body-mass index, renal status, and cardiopulmonary status affect the choice between pancreas or islet transplantation. Access to transplantation is limited by the number of deceased donors and the necessity of immunosuppression. Future approaches might include alternative sources of islets (eg, xenogeneic tissue or human stem cells), extrahepatic sites of implantation (eg, omental, subcutaneous, or intramuscular), and induction of immune tolerance or encapsulation of islets.
Copyright © 2019 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests
M-CV reports non-financial support from Novartis and Ipsen; personal fees from Sanofi, Aegerion, and GlaxoSmithKline; and participation in drug investigation trials supported by Shire and HRA Pharma, all outside the submitted work. MRR reports grants and personal fees from Xeris Pharmaceutical, personal fees from Hua Medicine, and non-financial support from Merck, all outside the submitted work. EJPdK and FP declare no competing interests.
Figures
Similar articles
-
Transplant strategies for type 1 diabetes: whole pancreas, islet and porcine beta cell therapies.Diabetologia. 2020 Oct;63(10):2049-2056. doi: 10.1007/s00125-020-05184-7. Epub 2020 Sep 7. Diabetologia. 2020. PMID: 32894315 Review.
-
[Islet transplantation in type I diabetes mellitus].Ther Umsch. 2005 Jul;62(7):481-6. doi: 10.1024/0040-5930.62.7.481. Ther Umsch. 2005. PMID: 16075955 Review. German.
-
Accessory cells for β-cell transplantation.Diabetes Obes Metab. 2016 Feb;18(2):115-24. doi: 10.1111/dom.12556. Epub 2015 Oct 9. Diabetes Obes Metab. 2016. PMID: 26289770 Review.
-
Current indications for pancreas or islet transplant.Diabetes Obes Metab. 2006 Jan;8(1):1-7. doi: 10.1111/j.1463-1326.2004.00460.x. Diabetes Obes Metab. 2006. PMID: 16367876 Review.
-
Islet cell transplantation.Curr Opin Organ Transplant. 2008 Dec;13(6):633-8. doi: 10.1097/MOT.0b013e328317a48b. Curr Opin Organ Transplant. 2008. PMID: 19060555 Review.
Cited by
-
Enhancement of Subcutaneous Islet Transplant Performance by Collagen 1 Gel.Cell Transplant. 2024 Jan-Dec;33:9636897241283728. doi: 10.1177/09636897241283728. Cell Transplant. 2024. PMID: 39361612 Free PMC article.
-
Development and Application of a Semi quantitative Scoring Method for Ultrastructural Assessment of Acute Stress in Pancreatic Islets.Transplant Direct. 2021 Dec 16;8(1):e1271. doi: 10.1097/TXD.0000000000001271. eCollection 2022 Jan. Transplant Direct. 2021. PMID: 34934809 Free PMC article.
-
Oxygen dynamics and delivery strategies to enhance beta cell replacement therapy.Am J Physiol Cell Physiol. 2025 May 1;328(5):C1667-C1684. doi: 10.1152/ajpcell.00984.2024. Epub 2025 Apr 9. Am J Physiol Cell Physiol. 2025. PMID: 40204281 Free PMC article. Review.
-
The Noble and Often Nobel Role Played by Insulin-Focused Research in Modern Medicine.Diabetes Care. 2022 Jan 1;45(1):23-27. doi: 10.2337/dci21-0012. Diabetes Care. 2022. PMID: 34986255 Free PMC article. Review.
-
Association between primary graft function and 5-year outcomes of islet allogeneic transplantation in type 1 diabetes: a retrospective, multicentre, observational cohort study in 1210 patients from the Collaborative Islet Transplant Registry.Lancet Diabetes Endocrinol. 2023 Jun;11(6):391-401. doi: 10.1016/S2213-8587(23)00082-7. Epub 2023 Apr 24. Lancet Diabetes Endocrinol. 2023. PMID: 37105208 Free PMC article.
References
-
- Diabetes Control and Complications Trial and Epidemiology of Diabetes Interventions and Complications Research Group, Lachin, Genuth S, Cleary P, Davis MD, Nathan DM Retinopathy and nephropathy in patients with type 1 diabetes four years after a trial of intensive therapy. N Engl J Med 2000; 342: 381–89. - PMC - PubMed
-
- Skrivarhaug T, Bangstad HJ, Stene LC, Sandvik L, Hanssen KF, Joner G. Long-term mortality in a nationwide cohort of childhood-onset type 1 diabetic patients in Norway. Diabetologia 2006; 49: 298–305. - PubMed
-
- Gruessner AC, Gruessner RW. Long-term outcome after pancreas transplantation: a registry analysis. Curr Opin Organ Transplant 2016; 21: 377–85. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
