

Transanal versus laparoscopic total mesorectal excision for mid and low rectal cancer: a meta-analysis of short-term outcomes
- PMID: 31534564
- PMCID: PMC6748052
- DOI: 10.5114/wiitm.2019.82798
Transanal versus laparoscopic total mesorectal excision for mid and low rectal cancer: a meta-analysis of short-term outcomes
Abstract
Introduction: The benefit of transanal total mesorectal excision (TaTME) for mid and low rectal cancer is conflicting.
Aim: To assess and compare the short-term outcomes of TaTME with conventional laparoscopic total mesorectal excision (LaTME) for middle and low rectal cancer.
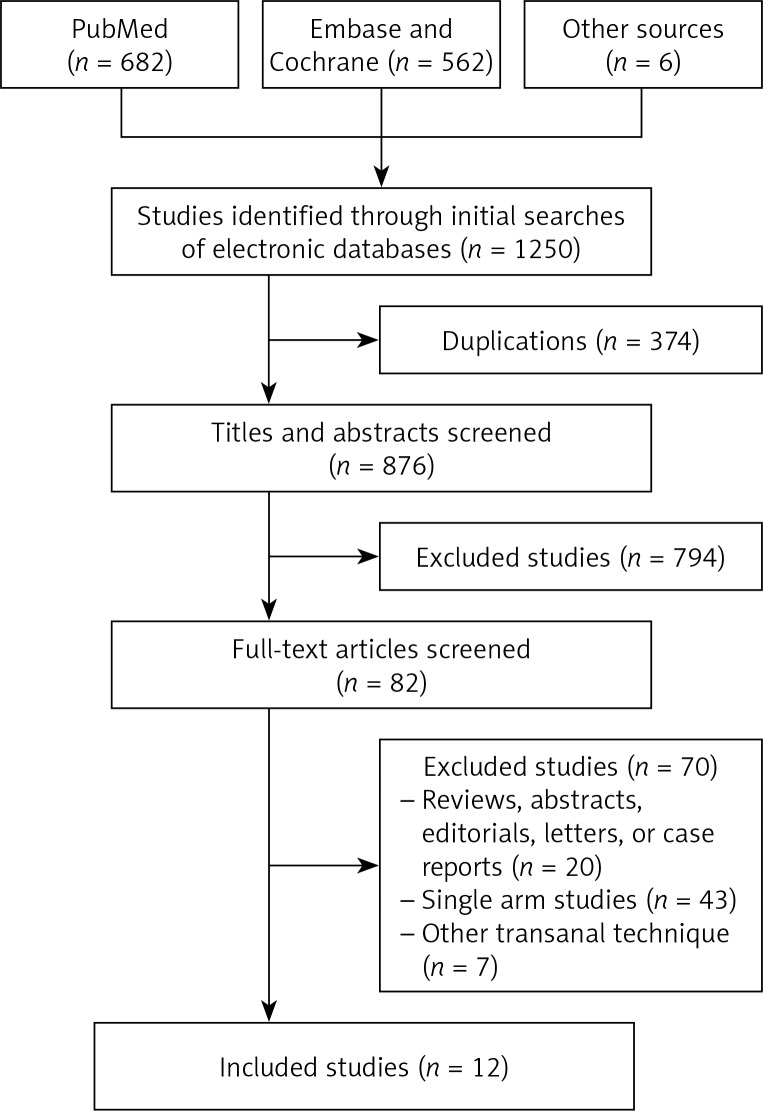
Material and methods: We searched PubMed, Embase and Cochrane Library databases for studies addressing TaTME versus conventional LaTME for rectal cancer between 2008 and December 2018. Randomized controlled trials (RCTs) and retrospective studies which compared TaTME with LaTME were included.
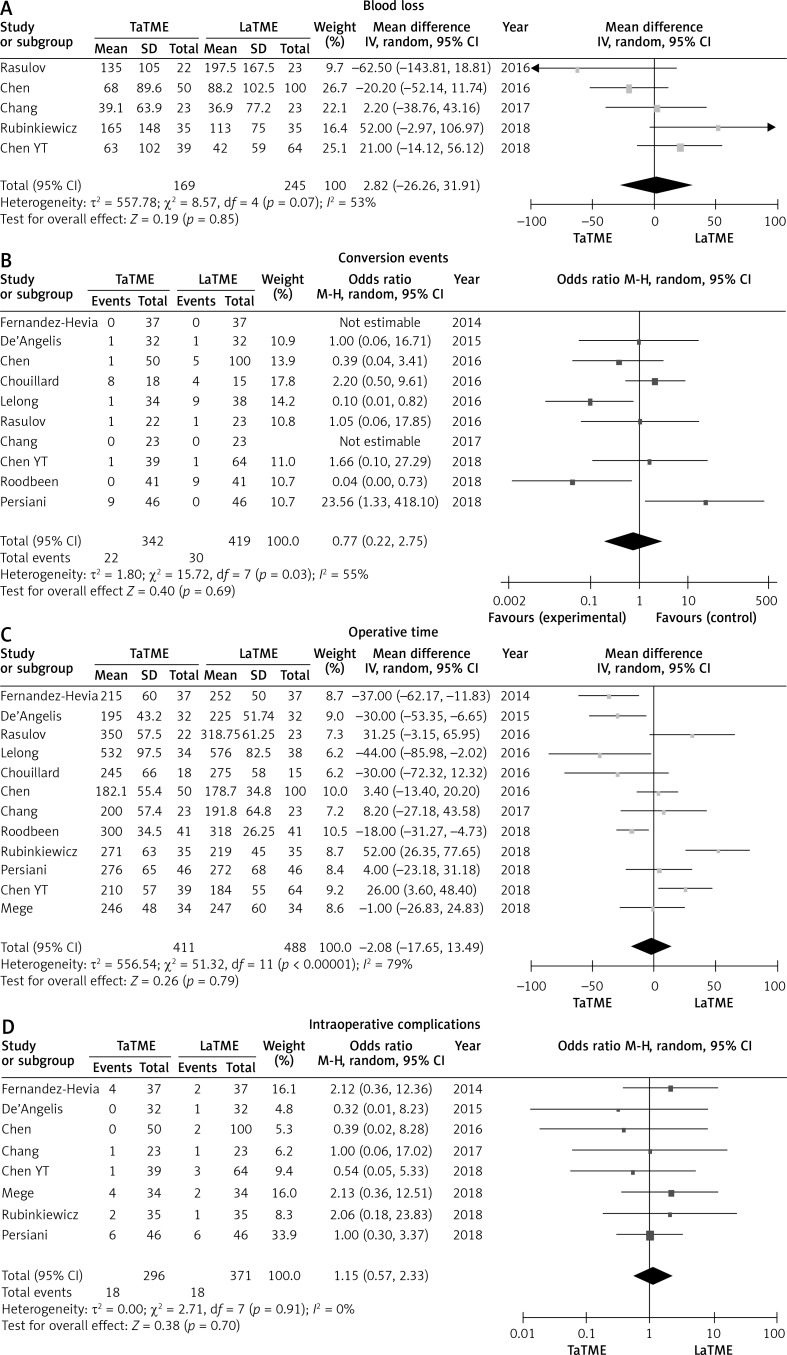
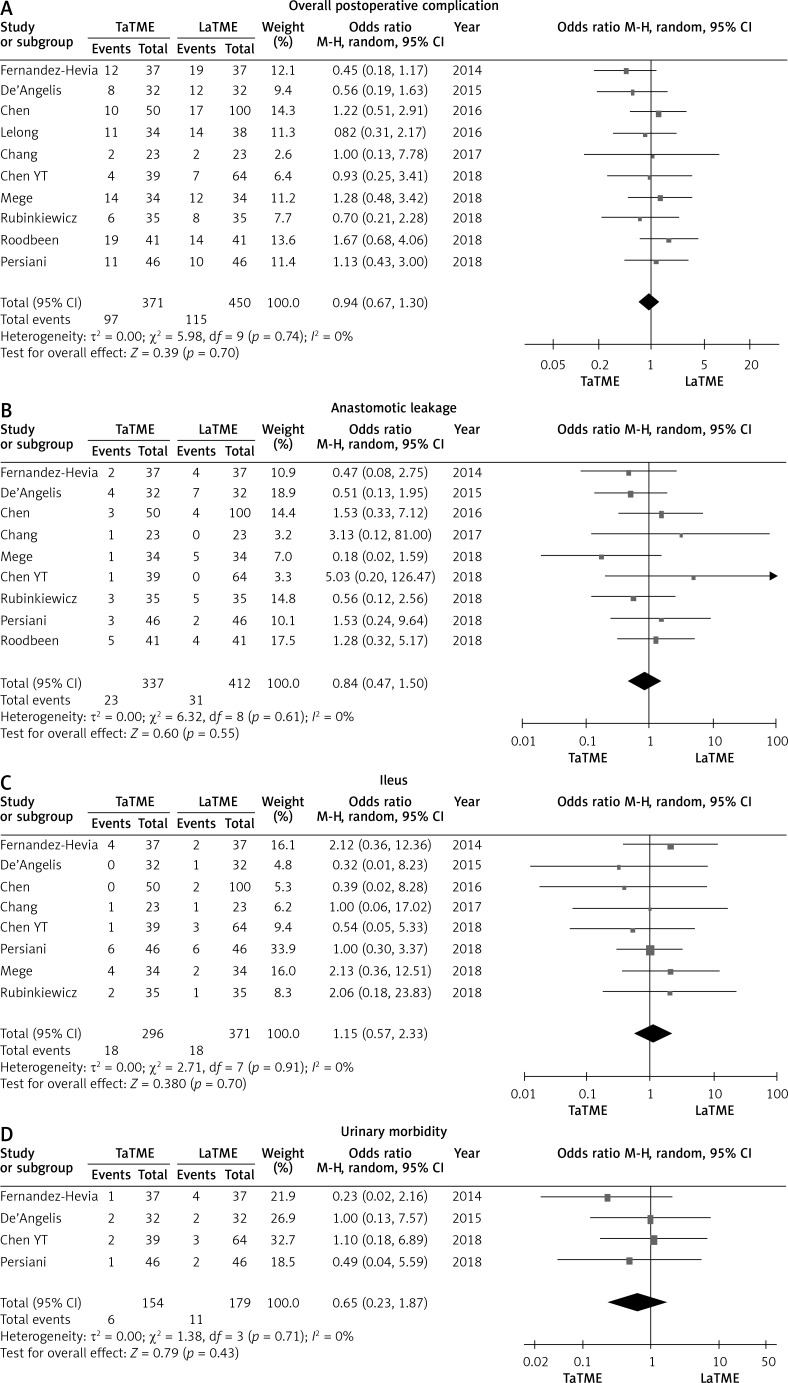
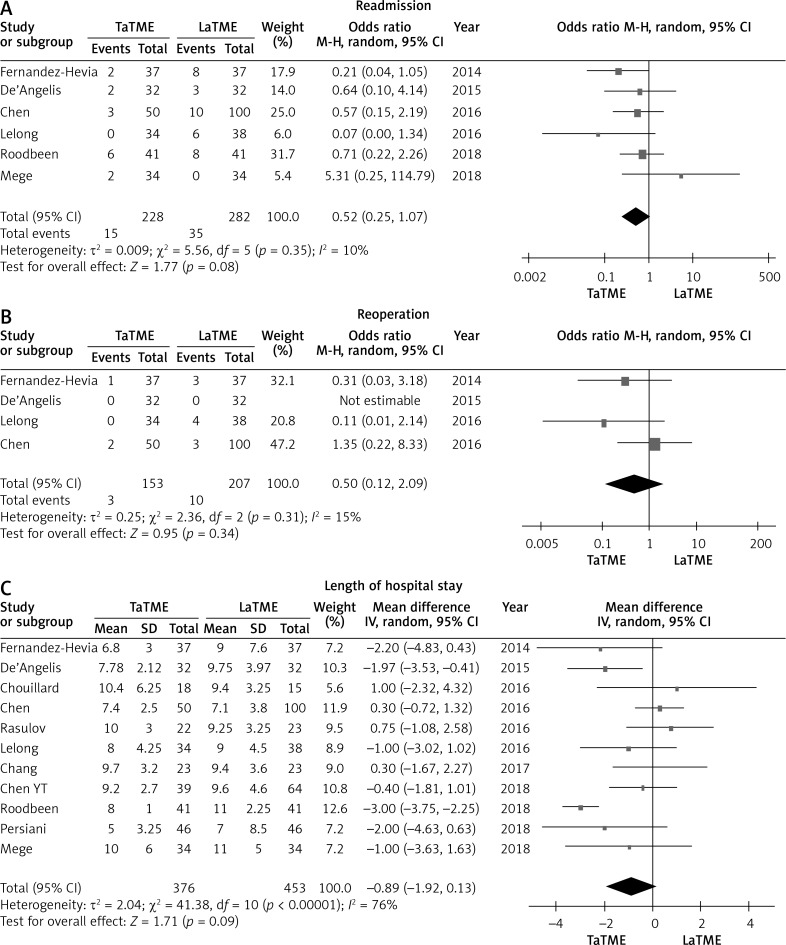
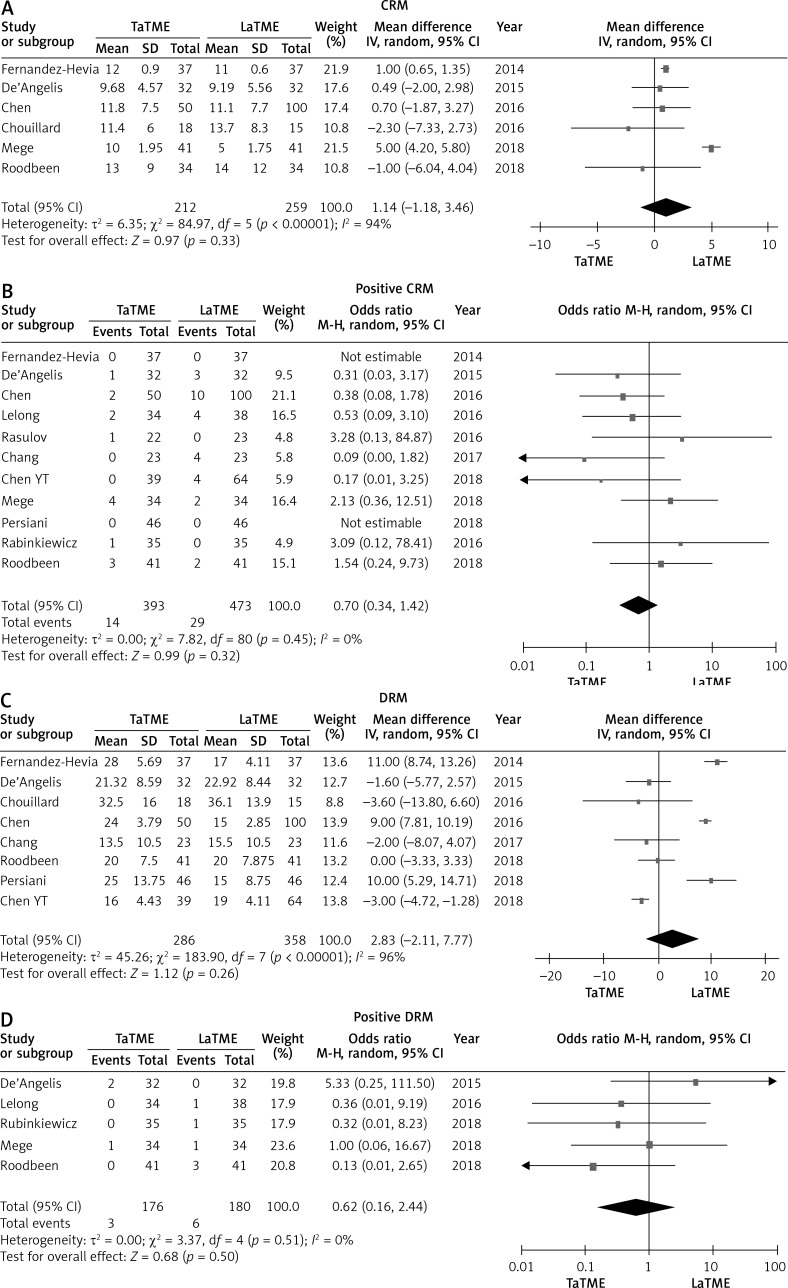
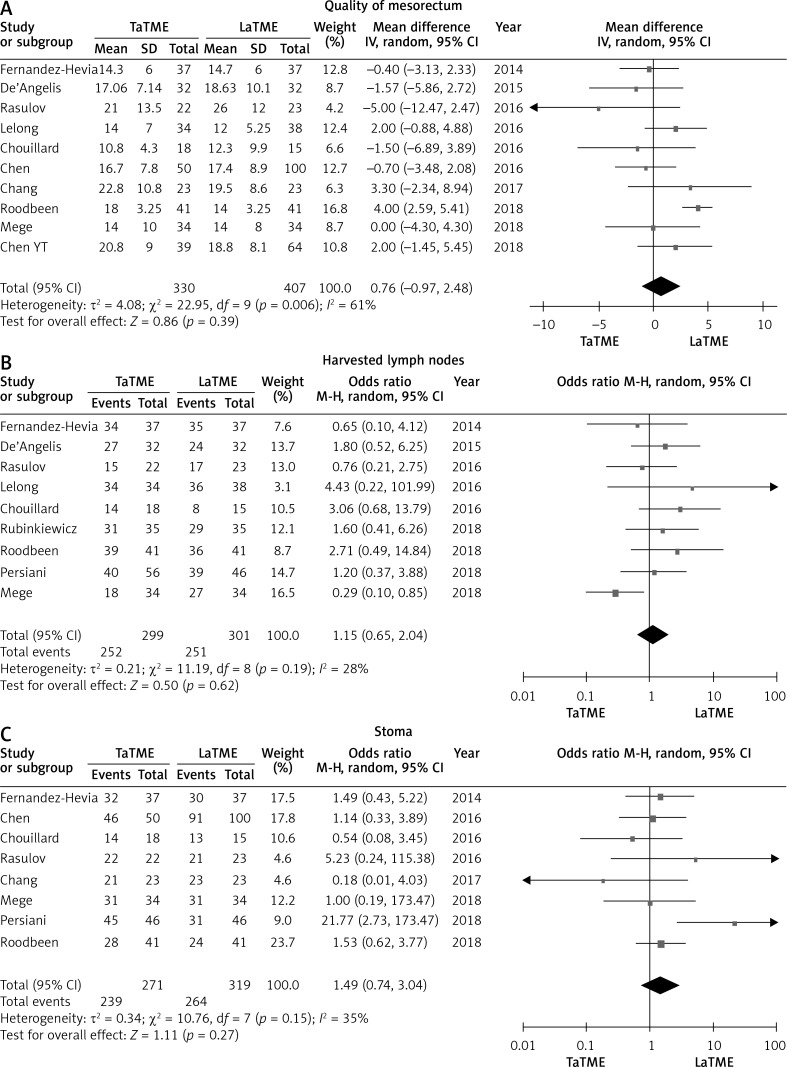
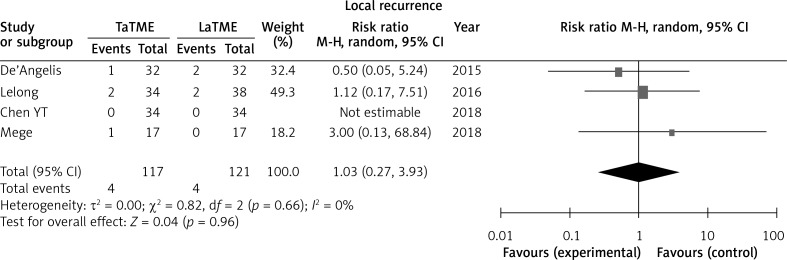
Results: Twelve retrospective case-control studies were identified, including a total of 899 patients. We did not find significant differences in overall intraoperative complications, blood loss, conversion rate, operative time, overall postoperative complication, anastomotic leakage, ileus, or urinary morbidity. Also no significant differences in oncological outcomes including circumferential resection margin (CRM), positive CRM, distal margin distance (DRM), positive DRM, quality of mesorectum, number of harvested lymph nodes, temporary stoma or local recurrence were found. Although the TaTME group had better postoperative outcomes (readmission, reoperation, length of hospital stay) on average, the difference did not reach statistical significance.
Conclusions: Transanal total mesorectal excision offers a safe and feasible alternative to LaTME although the clinicopathological features were not superior to LaTME in this study. Currently, with the lack of evidence on benefits of TaTME, further evaluation of TaTME requires large randomized control trials to be conducted.
Keywords: laparoscopic total mesorectal excision; meta-analysis; rectal cancer; transanal total mesorectal excision.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Ries LA, Wingo PA, Miller DS, et al. The annual report to the nation on the status of cancer, 1973-1997, with a special section on colorectal cancer. Cancer. 2000;88:2398–424. - PubMed
-
- Jacobs M, Verdeja JC, Goldstein HS. Minimally invasive colon resection (laparoscopic colectomy) Surg Laparosc Endosc. 1991;1:144–50. - PubMed
-
- Kearney DE, Coffey JC. A Randomized trial of laparoscopic versus open surgery for rectal cancer. N Engl J Med. 2015;373:194. - PubMed
-
- Jeong SY, Park JW, Nam BH, et al. Open versus laparoscopic surgery for mid-rectal or low-rectal cancer after neoadjuvant chemoradiotherapy (COREAN trial): survival outcomes of an open-label, non-inferiority, randomised controlled trial. Lancet Oncol. 2014;15:767–74. - PubMed
LinkOut - more resources
Full Text Sources