

Minimally-Invasive midline posterior interbody fusion with cortical bone trajectory screws compares favorably to traditional open transforaminal interbody fusion
- PMID: 31535047
- PMCID: PMC6744604
- DOI: 10.1016/j.heliyon.2019.e02423
Minimally-Invasive midline posterior interbody fusion with cortical bone trajectory screws compares favorably to traditional open transforaminal interbody fusion
Abstract
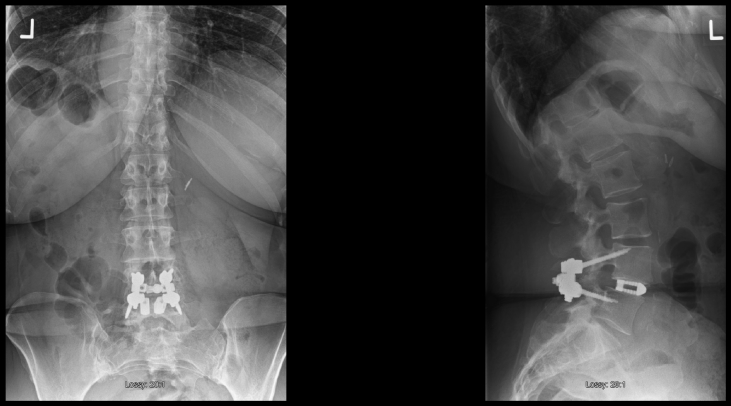
Objective: Posterior interbody fusion is commonly performed for degenerative lumbar conditions. A minimally invasive technique of midline exposure limited only to the facets and fixation with laterally directed cortical bone trajectory (CBT) screws was introduced with the intent of decreasing surgical morbidity. The purpose of this study was to determine if posterior interbody fusion with this limited midline exposure will have less blood loss and shorter operative times (i.e., can be considered minimally invasive) compared to traditional open transforaminal interbody fusion.
Methods: A consecutive single-surgeon series of patients who underwent posterior interbody fusion with either a navigated, midline only exposure (MidLIF) or full, traditional open, exposure of the transverse processes with a posterolateral fusion (open TLIF) were identified. Demographic, peri-operative data, patient reported outcomes (PROs), and reoperation/readmission rates were collected and compared.
Results: There were 29 cases in the MidLIF and 27 in the open TLIF group. Both groups were similar with respect to surgical indications, age, BMI, gender, ASA grade and operative level. The MidLIF group had significantly lower estimated blood loss (266 vs. 446 cc, p = 0.003), shorter operative time (170 vs. 210 minutes, p = 0.003), and shorter length of hospital stay (2.9 vs. 3.7 days, p = 0.016) compared to the open TLIF group. A sub-analysis of single-level cases showed similar findings with significantly lower estimated blood loss (247 vs. 411 cc, p = 0.10), shorter operative time (159 vs. 199 min, p = 0.003), and shorter length of hospital stay (2.9 vs. 3.7 days, p = 0.023) in the MidLIF group. Patient reported outcomes at 6 weeks, 3 months, 6 months, 12 months and 24 months post-operative favored MidLIF with significantly greater ODI improvements at both 6 weeks and 12 months; and lower ODI and back pain at both 12 months and 24 months.
Conclusions: MidLIF had lower blood loss and shorter operative time compared to the traditional open TLIF technique. These differences compare well to reported values in the literature for tubular minimally-invasive TLIF. Patient reported outcomes from 6 weeks to 24 months post-operative, hospital length of stay, and reoperation/readmission rates all favored MidLIF compared to traditional open TLIF.
Keywords: Lumbar degenerative disease; Medicine; Midline interbody fusion; Neurology; Surgery; Transforaminal interbody fusion.
Figures

References
-
- Mirza S.K., Deyo R.A., Heagerty P.J., Konodi M.A., Lee L.A., Turner J.A. Development of an index to characterize the "invasiveness" of spine surgery: validation by comparison to blood loss and operative time. Spine (Phila Pa 1976) 2008 Nov 15;33(24):2651–2661. - PubMed
-
- Wu W.C., Smith T.S., Henderson W.G., Eaton C.B., Poses R.M., Uttley G. Operative blood loss, blood transfusion, and 30-day mortality in older patients after major noncardiac surgery. Ann. Surg. 2010 Jul;252(1):11–17. - PubMed
-
- Canan C.E., Myers J.A., Owens R.K., Crawford C.H., 3rd, Djurasovic M., Burke L.O. Blood salvage produces higher total blood product costs in single-level lumbar spinal surgery. Spine (Phila Pa 1976) 2013 Apr 15;38(8):703–708. - PubMed
-
- Owens R.K., Crawford C.H., 3rd, Djurasovic M., Canan C.E., Burke L.O., Bratcher K.R. Predictive factors for the use of cell saver in lumbar spinal surgery. Spine (Phila Pa 1976) 2013 Feb 15;38(4):E217–E222. - PubMed
-
- Goldstein C.L., Macwan K., Sundararajan K., Rampersaud Y.R. Perioperative outcomes and adverse events of minimally invasive versus open posterior lumbar fusion: meta-analysis and systematic review. J. Neurosurg. Spine. 2016;24:416–427. - PubMed
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
