

Association Between Pain and Patient Satisfaction After Rhinoplasty
- PMID: 31536105
- PMCID: PMC6753502
- DOI: 10.1001/jamafacial.2019.0808
Association Between Pain and Patient Satisfaction After Rhinoplasty
Abstract
Importance: In light of the current opioid crisis, there exists a demonstrated need to balance adequate postrhinoplasty pain control with measured use of narcotics. If pain is inadequately controlled, patients may be unsatisfied with their elective surgical experience.
Objectives: To characterize the association between patient-reported pain outcomes, objective opioid use, and perception of surgical success.
Design, setting, and participants: A case series survey study was conducted from July 2018 to January 2019. Consecutive patients who underwent cosmetic and/or functional rhinoplasty by 2 facial plastic surgeons (D.A.S. and L.N.L.) at an academic medical center were surveyed 1 month after surgery.
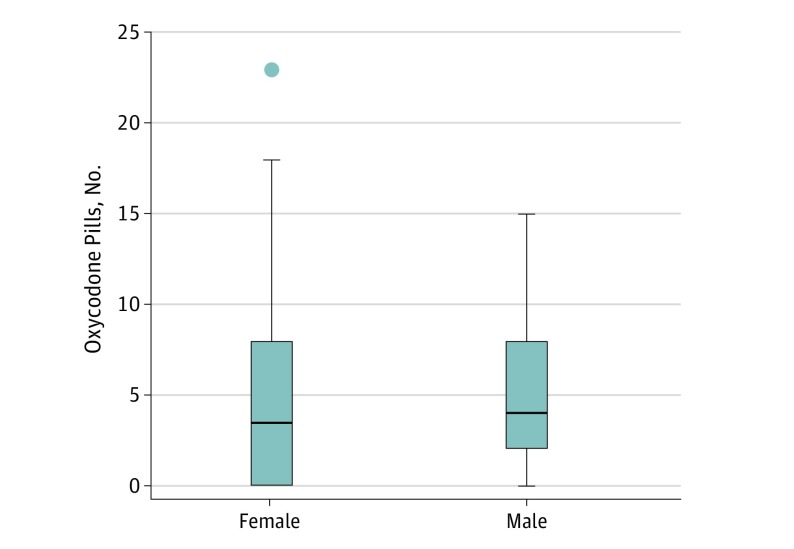
Main outcomes and measures: The number of oxycodone tablets taken, patient-reported pain outcomes, number of narcotic prescription refills, and patient-reported functional and cosmetic outcomes were recorded. Perception of pain, surgical outcome, and oxycodone intake were also evaluated by sex. Demographic information and perception of surgical results were recorded. Statistical analysis was performed using STATA statistical software (version 12.0, STATA Corp). Spearman rank order correlation was used for ordinal, monotonic variables with P < .05 being considered statistically significant.
Results: Overall, 104 patients were surveyed; 6 were lost to follow-up. Of the participants included, 50 were women with a mean (SD) age of 38 (16.0) years and 48 were men with a mean (SD) age of 38 (16.7) years. Although patients were prescribed a range of 10 to 40 tablets of oxycodone, patients took a mean (SD) of 5.2 tablets (range, 0-23). There were no significant sex differences in perception of pain, perception of outcome, or narcotic use. Among patients undergoing purely functional rhinoplasty, a statistically significant negative association between perception of pain and perception of functional outcome (breathing improvement) was evident. Patients who experienced less pain than they expected had a greater perception of functional improvement (rs = -0.62, P = .001). In contrast, among patients who underwent rhinoplasty with cosmetic improvement, no association was found between pain and perception of surgical outcome (rs = 0.05, P = .64).
Conclusions and relevance: To our knowledge, this is the first study to prospectively evaluate the association between opioid use, patient-reported pain, and perceived surgical success. These data may help guide preoperative counseling because patients who are interested purely in breathing improvement (without cosmetic change) may warrant additional pain-specific counseling to optimize patient satisfaction.
Level of evidence: 3.
Conflict of interest statement
Figures

Similar articles
-
Opioid Use by Patients After Rhinoplasty.JAMA Facial Plast Surg. 2018 Jan 1;20(1):24-30. doi: 10.1001/jamafacial.2017.1034. JAMA Facial Plast Surg. 2018. PMID: 29121158 Free PMC article.
-
Prospective Qualitative Multidimensional Assessment of the Postoperative Rhinoplasty Experience.Facial Plast Surg Aesthet Med. 2020 May/Jun;22(3):213-218. doi: 10.1089/fpsam.2020.0047. Epub 2020 Mar 30. Facial Plast Surg Aesthet Med. 2020. PMID: 32223570
-
Defining Typical Acetaminophen and Narcotic Usage in the Postoperative Rhinoplasty Patient.Laryngoscope. 2021 Jan;131(1):48-53. doi: 10.1002/lary.28531. Epub 2020 Feb 7. Laryngoscope. 2021. PMID: 32031696
-
Oral Oxycodone for Acute Postoperative Pain: A Review of Clinical Trials.Pain Physician. 2017 Feb;20(2S):SE33-SE52. Pain Physician. 2017. PMID: 28226340 Review.
-
Observer-Reported Outcomes and Cosmetic Procedures: A Systematic Review.Dermatol Surg. 2021 Jan 1;47(1):65-69. doi: 10.1097/DSS.0000000000002496. Dermatol Surg. 2021. PMID: 32769529
Cited by
-
No Opioids after Septorhinoplasty: A Multimodal Analgesic Protocol.Plast Reconstr Surg Glob Open. 2020 Dec 21;8(12):e3305. doi: 10.1097/GOX.0000000000003305. eCollection 2020 Dec. Plast Reconstr Surg Glob Open. 2020. PMID: 33425613 Free PMC article.
-
Dexmedetomidine versus remifentanil in nasal surgery: a systematic review and meta-analysis.BMC Anesthesiol. 2024 May 30;24(1):194. doi: 10.1186/s12871-024-02563-0. BMC Anesthesiol. 2024. PMID: 38816731 Free PMC article.
-
Effect of a Single Preventive Intravenous Dose of Ketorolac and Paracetamol on Reducing Postoperative Pain in Septorhinoplasty Patients: Double-Blind Randomized Clinical Trial.Iran J Med Sci. 2025 Apr 1;50(4):239-246. doi: 10.30476/ijms.2024.102131.3488. eCollection 2025 Apr. Iran J Med Sci. 2025. PMID: 40255229 Free PMC article. Clinical Trial.
-
Evaluating the Efficacy of Liposomal Bupivacaine in Postoperative Pain Management for Rhinoplasty: A Retrospective Study.Aesthetic Plast Surg. 2024 May;48(9):1722-1727. doi: 10.1007/s00266-023-03656-w. Epub 2023 Sep 29. Aesthetic Plast Surg. 2024. PMID: 37775576
-
Comparison of Outcomes After Septoplasty With Non-Absorbable or Biodegradable Synthetic Polyurethane Foam Nasal Packing With a Focus on Pain and Cardiac Factors.J Rhinol. 2023 Mar;30(1):31-36. doi: 10.18787/jr.2023.00005. Epub 2023 Mar 30. J Rhinol. 2023. PMID: 39664705 Free PMC article.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials