

Occurrence and Practices for Pain, Agitation, and Delirium in Intensive Care Unit Patients
- PMID: 31536628
- PMCID: PMC6906604
Occurrence and Practices for Pain, Agitation, and Delirium in Intensive Care Unit Patients
Abstract
Objective: Our study described the occurrence, assessment, prevention, and management practices of pain, agitation, and delirium (PAD) in four intensive care units (ICUs) from the Puerto Rico Medical Center and compared findings with the 2013 PAD guidelines.
Methods: A descriptive study, with repeated bedside measures (two times a day/two times a week) of PAD and review of patient clinical records.
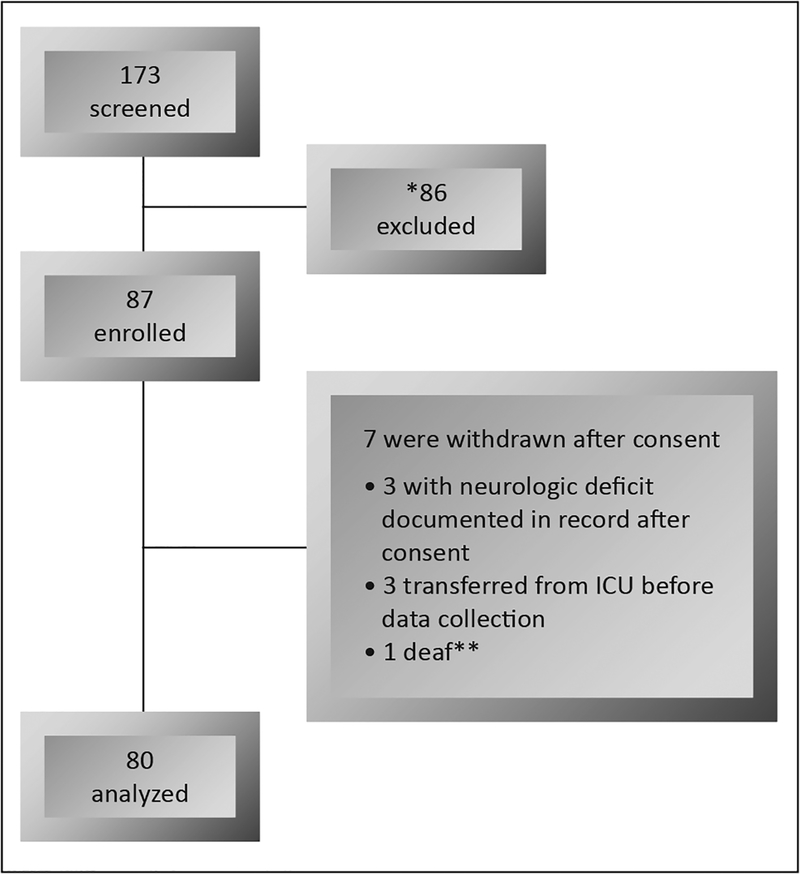
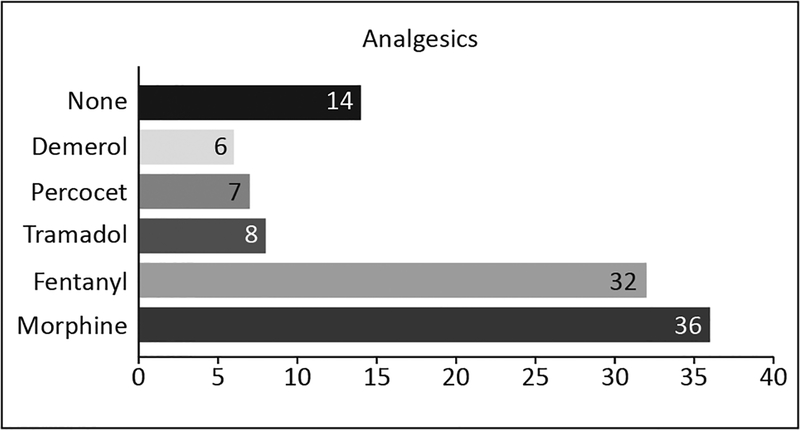
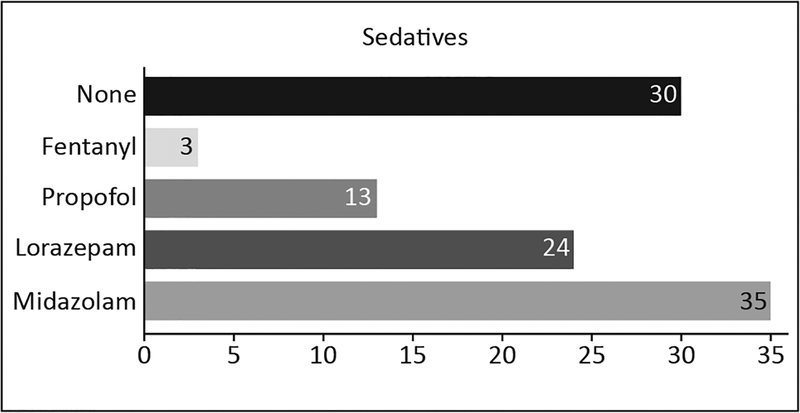
Results: Eighty ICU patients (20 per ICU) were evaluated, (median 3 times [IQR, 2-7]). At least once during the assessment period, 57% percent of patients had significant pain and 34% had delirium. Moreover, 46% were deeply sedated, 17.5% had agitation, and 52.5% of patients were within the recommended Richmond Agitation-Sedation Scale (RASS) scores. The Numeric Rating Scale and RASS were the most common tools used by clinicians to evaluate pain and agitation/sedation levels, respectively. Clinicians did not assess pain in patients unable to self-report with any guideline-recommended tools, as was the case for delirium. Fentanyl and morphine were the most commonly used analgesics, while benzodiazepines were used for sedation.
Conclusion: Although pain, agitation, and delirium occurrence were similar to other studies, patients continue to suffer. A gap exists between clinical practices in these ICUs and current guidelines. Strategies that contribute to integrating guidelines into these ICUs should be developed, studied, and implemented.
Objetivos:: Se describió la ocurrencia, estimado, prevención y prácticas de manejo de dolor, agitación y delirium (DAD) en cuatro unidades de cuidado intensivo (UCI) del Centro Médico de Puerto Rico y comparó los hallazgos con las guías de DAD del 2013.
Metodología:: Estudio descriptivo con medidas repetidas (dos veces al día/dos veces en semana) de DAD y la revisión de expedientes clínicos.
Resultados:: Ochenta pacientes de UCI (20/unidad) fueron evaluados (mediana 3 veces, [IQR, 2–7]). Al menos una vez durante el periodo de estimado, el 57% de los pacientes tenía dolor significativo y el 34% tenía delirium. Además, el 46% estaba profundamente sedado, el 17.5% tenía agitación y el 52.5% de los pacientes se encontraban dentro de los niveles recomendados en la Escala de Agitación-Sedación de Richmond (RASS). La Escala de Valoración Numérica y el RASS fueron las herramientas más comúnmente utilizadas por los clínicos para evaluar los niveles de dolor y agitación/sedación, respectivamente. Los clínicos no evaluaron el dolor en pacientes incapaces de auto-reportarlo usando instrumentos recomendados por las guías, como fue el caso con el delirium. El fentanilo y la morfina fueron los medicamentos más utilizados para la analgesia, mientras que las benzodiacepinas se utilizaron para la sedación.
Conclusiones:: Aunque la ocurrencia de DAD es similar a otros estudios, los pacientes continúan sufriendo estos fenómenos. Existe una brecha entre las prácticas clínicas de las UCI y las guías actuales. Se deben desarrollar, estudiar e implementar estrategias que contribuyan a la integración de estas guías en las UCI.
Keywords: Agitation; Analgesia; Delirium; Intensive care unit; Pain; Sedation.
Conflict of interest statement
The author/s has/have no conflict/s of interest to disclose. This study was funded by Capacity Advancement in Research Infrastructure University of Puerto Rico UPR MFP-6251123.
Figures
References
-
- Payen J-F, Chanques G, Mantz J, Hercule C, Auriant I, Leguillou J-L, et al. Current practices in sedation and analgesia for mechanically ventilated critically ill patients: a prospective multicenter patient-based study. Anesthesiology 2007;106:687–695. - PubMed
-
- Chanques G, Sebbane M, Barbotte E, Viel E, Eledjam J-J, Jaber S. A prospective study of pain at rest: incidence and characteristics of an unrecognized symptom in surgical and trauma versus medical intensive care unit patients. Anesthesiology 2007;107:858–860. - PubMed
-
- Jaber S, Chanques G, Altairac C, Sebbane M, Vergne C, Perrigault P-F, et al. A prospective study of agitation in a medical-surgical ICU: Incidence, risk factors, and outcomes. Chest. 2005;128:2749–57. - PubMed
-
- Bigatello LM, Amirfarzan H, Haghighi AK, Newhouse B, Del Rio JM, Allen K, et al. Effects of routine monitoring of delirium in a surgical/trauma intensive care unit. J Trauma Acute Care Surg 2013;74:876–883. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous