

Male contraception: where are we going and where have we been?
- PMID: 31537614
- PMCID: PMC6892591
- DOI: 10.1136/bmjsrh-2019-200395
Male contraception: where are we going and where have we been?
Erratum in
-
Correction: Male contraception: where are we going and where have we been?.BMJ Sex Reprod Health. 2020 Apr;46(2):157. doi: 10.1136/bmjsrh-2019-200395corr1. BMJ Sex Reprod Health. 2020. PMID: 32303626 Free PMC article. No abstract available.
Abstract
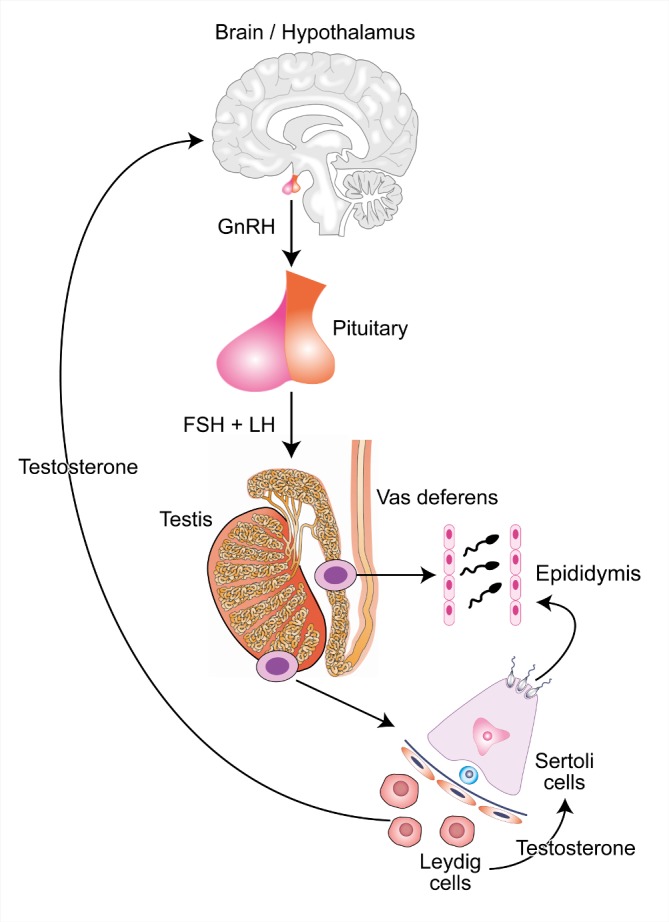
Progress in developing new reversible male contraception has been slow. While the hormonal approach has been clearly shown to be capable of providing effective and reversible contraception, there remains no product available. Currently, trials of a self-administered gel combination of testosterone and the progestogen Nestorone® are under way, complementing the largely injectable methods previously investigated. Novel long-acting steroids with both androgenic and progestogenic activity are also in early clinical trials. The non-hormonal approach offers potential advantages, with potential sites of action on spermatogenesis, and sperm maturation in the epididymis or at the vas, but remains in preclinical testing. Surveys indicate the willingness of men, and their partners, to use a new male method, but they continue to lack that opportunity.
Keywords: hormonal contraception; male contraception; review.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Faculty of Sexual and Reproductive Healthcare Better care, a better future: a new vision for sexual and reproductive health care in the UK, 2015. Available: https://www.fsrh.org/documents/fsrh-vision/
-
- Coviello AD, Bremner WJ, Matsumoto AM, et al. . Intratesticular testosterone concentrations comparable with serum levels are not sufficient to maintain normal sperm production in men receiving a hormonal contraceptive regimen. J Androl 2004;25:931–8. 10.1002/j.1939-4640.2004.tb03164.x - DOI - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources