

Sequential screening for lung cancer in a high-risk group: randomised controlled trial: LungSEARCH: a randomised controlled trial of Surveillance using sputum and imaging for the EARly detection of lung Cancer in a High-risk group
- PMID: 31537697
- PMCID: PMC6796151
- DOI: 10.1183/13993003.00581-2019
Sequential screening for lung cancer in a high-risk group: randomised controlled trial: LungSEARCH: a randomised controlled trial of Surveillance using sputum and imaging for the EARly detection of lung Cancer in a High-risk group
Abstract
Background: Low-dose computed tomography (LDCT) screening detects early-stage lung cancer and reduces mortality. We proposed a sequential approach targeted to a high-risk group as a potentially efficient screening strategy.
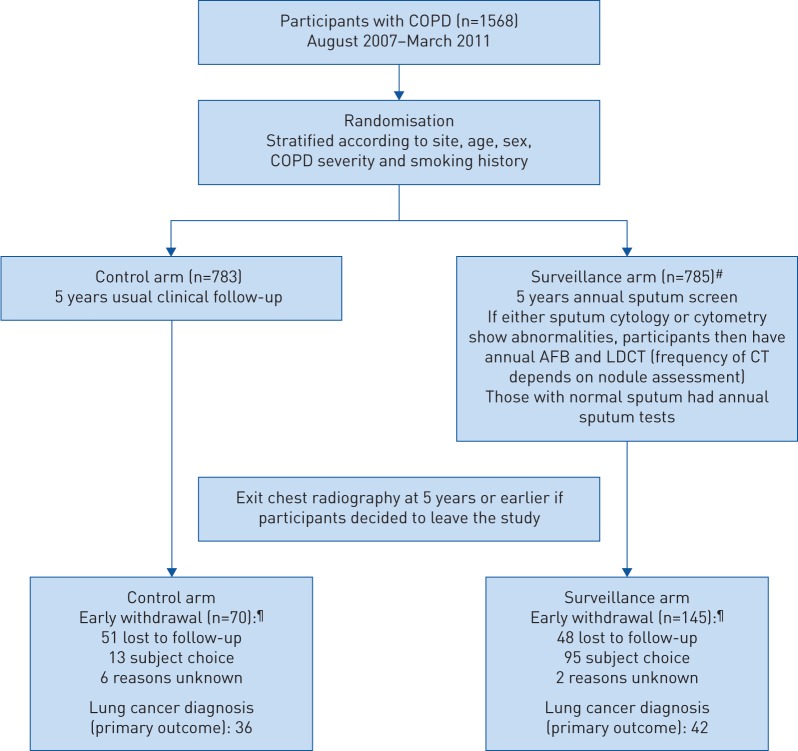
Methods: LungSEARCH was a national multicentre randomised trial. Current/ex-smokers with mild/moderate chronic obstructive pulmonary disease (COPD) were allocated (1:1) to have 5 years surveillance or not. Screened participants provided annual sputum samples for cytology and cytometry, and if abnormal were offered annual LDCT and autofluorescence bronchoscopy (AFB). Those with normal sputum provided annual samples. The primary end-point was the percentage of lung cancers diagnosed at stage I/II (nonsmall cell) or limited disease (small cell).
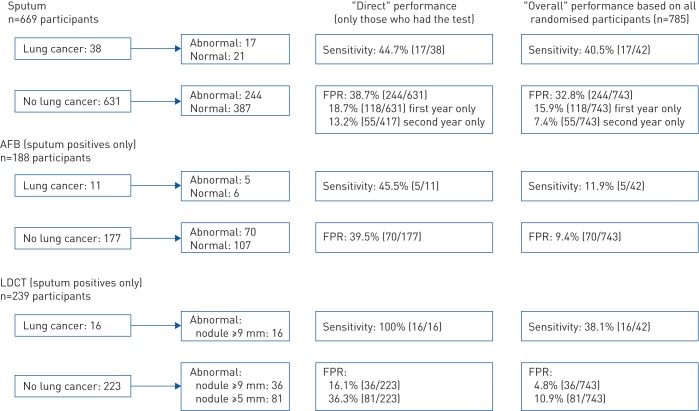
Results: 1568 participants were randomised during 2007-2011 from 10 UK centres. 85.2% of those screened provided an adequate baseline sputum sample. There were 42 lung cancers among 785 screened individuals and 36 lung cancers among 783 controls. 54.8% (23 out of 42) of screened individuals versus 45.2% (14 out of 31) of controls with known staging were diagnosed with early-stage disease (one-sided p=0.24). Relative risk was 1.21 (95% CI 0.75-1.95) or 0.82 (95% CI 0.52-1.31) for early-stage or advanced cancers, respectively. Overall sensitivity for sputum (in those randomised to surveillance) was low (40.5%) with a cumulative false-positive rate (FPR) of 32.8%. 55% of cancers had normal sputum results throughout. Among sputum-positive individuals who had AFB, sensitivity was 45.5% and cumulative FPR was 39.5%; the corresponding measures for those who had LDCT were 100% and 16.1%, respectively.
Conclusions: Our sequential strategy, using sputum cytology/cytometry to select high-risk individuals for AFB and LDCT, did not lead to a clear stage shift and did not improve the efficiency of lung cancer screening.
Copyright ©ERS 2019.
Conflict of interest statement
Conflict of interest: S.G. Spiro has nothing to disclose. Conflict of interest: P.L. Shah has nothing to disclose. Conflict of interest: R.C. Rintoul has nothing to disclose. Conflict of interest: J. George has nothing to disclose. Conflict of interest: S. Janes reports personal fees for advisory board work from BARD1, Achilles Therapeutics and AstraZeneca, personal fees for conference travel from AstraZeneca, outside the submitted work. Conflict of interest: M. Callister has nothing to disclose. Conflict of interest: M. Novelli has nothing to disclose. Conflict of interest: P. Shaw has nothing to disclose. Conflict of interest: G. Kocjan has nothing to disclose. Conflict of interest: C. Griffiths has nothing to disclose. Conflict of interest: M. Falzon has nothing to disclose. Conflict of interest: R. Booton has nothing to disclose. Conflict of interest: N. Magee has nothing to disclose. Conflict of interest: M. Peake reports personal fees for lectures from Roche Products Ltd, grants and personal fees for lectures from MSD Ltd, personal fees for advisory board work from BMS and Pfizer Ltd, outside the submitted work. Conflict of interest: P. Dhillon has nothing to disclose. Conflict of interest: K. Sridharan has nothing to disclose. Conflict of interest: A.G. Nicholson has nothing to disclose. Conflict of interest: S. Padley has nothing to disclose. Conflict of interest: M.N. Taylor has nothing to disclose. Conflict of interest: A. Ahmed has nothing to disclose. Conflict of interest: J. Allen has nothing to disclose. Conflict of interest: Y. Ngai has nothing to disclose. Conflict of interest: N. Chinyanganya has nothing to disclose. Conflict of interest: V. Ashford-Turner has nothing to disclose. Conflict of interest: S. Lewis has nothing to disclose. Conflict of interest: D. Oukrif has nothing to disclose. Conflict of interest: P. Rabbits has nothing to disclose. Conflict of interest: N. Counsell has nothing to disclose. Conflict of interest: A. Hackshaw has nothing to disclose.
Figures
References
-
- Office for National Statistics. Cancer survival in England: adult, stage at diagnosis and childhood – patients followed up to 2016. Cancer survival in England for specific cancer sites by age, sex and stage at diagnosis 2017. www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/conditio... Date last accessed: July 28, 2019.
-
- van Klaveren RJ, Oudkerk M, Prokop M, et al. Management of lung nodules detected by volume CT scanning. N Engl J Med 2009; 361: 2221–2229. - PubMed
-
- Bepler G, Carney DG, Djulbegovic B, et al. A systematic review and lessons learned from early lung cancer detection trials using low-dose computed tomography of the chest. Cancer Control 2003; 10: 306–314. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical