

Long-Term Corticosteroid-Sparing Immunosuppression for Cardiac Sarcoidosis
- PMID: 31538835
- PMCID: PMC6818011
- DOI: 10.1161/JAHA.118.010952
Long-Term Corticosteroid-Sparing Immunosuppression for Cardiac Sarcoidosis
Abstract
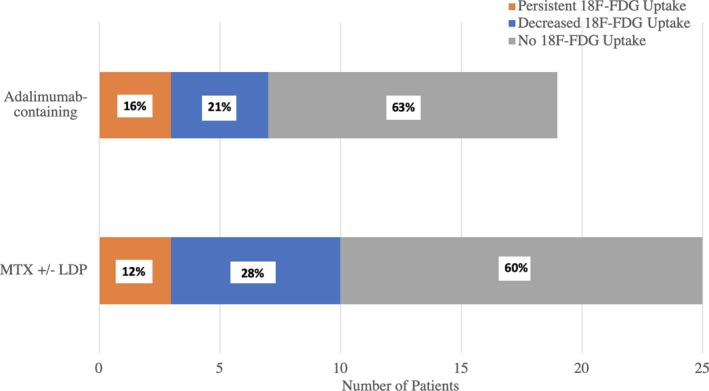
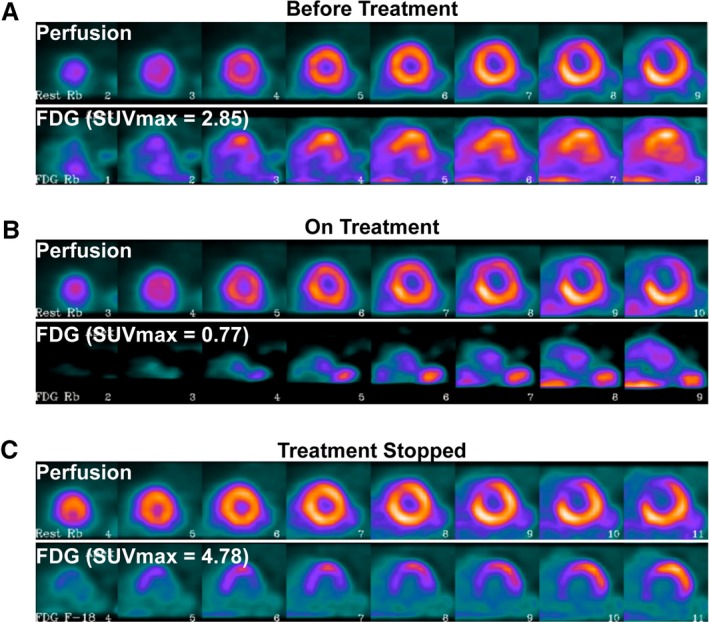
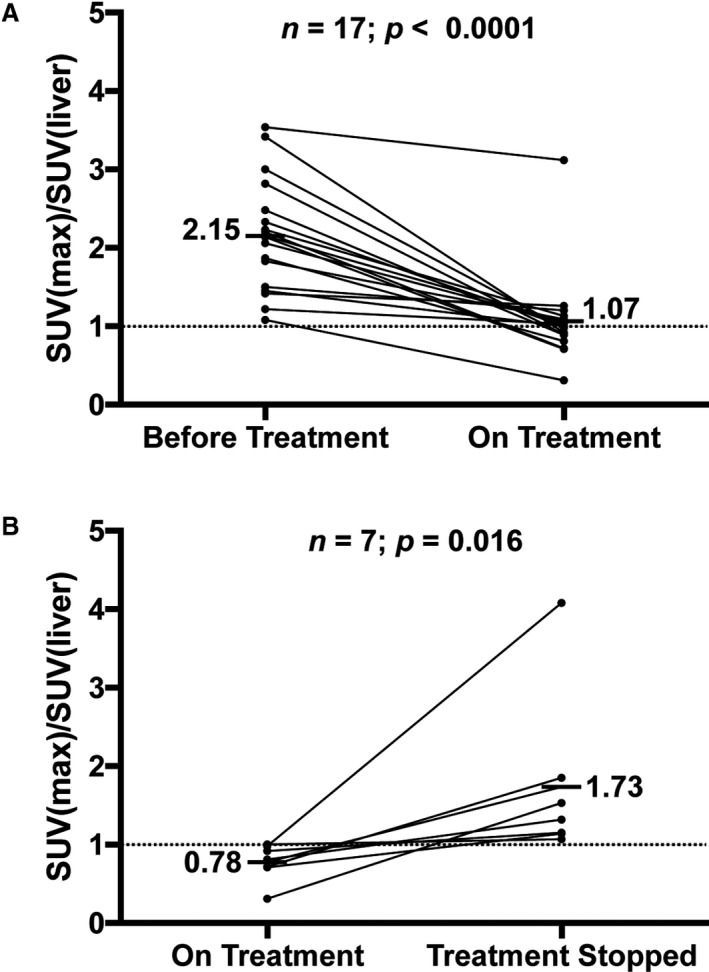
Background Long-term corticosteroid therapy is the standard of care for treatment of cardiac sarcoidosis (CS). The efficacy of long-term corticosteroid-sparing immunosuppression in CS is unknown. The goal of this study was to assess the efficacy of methotrexate with or without adalimumab for long-term disease suppression in CS, and to assess recurrence and adverse event rates after immunosuppression discontinuation. Methods and Results Retrospective chart review identified treatment-naive CS patients at a single academic medical center who received corticosteroid-sparing maintenance therapy. Demographics, cardiac uptake of 18-fluorodeoxyglucose, and adverse cardiac events were compared before and during treatment and between those with persistent or interrupted immunosuppression. Twenty-eight CS patients were followed for a mean 4.1 (SD 1.5) years. Twenty-five patients received 4 to 8 weeks of high-dose prednisone (>30 mg/day), followed by taper and maintenance therapy with methotrexate±low-dose prednisone (low-dose prednisone, <10 mg/day). Adalimumab was added in 19 patients with persistently active CS or in those with intolerance to methotrexate. Methotrexate±low-dose prednisone resulted in initial reduction (88%) or elimination (60%) of 18-fluorodeoxyglucose uptake, and patients receiving adalimumab-containing regimens experienced improved (84%) or resolved (63%) 18-fluorodeoxyglucose uptake. Radiologic relapse occurred in 8 of 9 patients after immunosuppression cessation, 4 patients on methotrexate-containing regimens, and in no patients on adalimumab-containing regimens. Conclusions Corticosteroid-sparing regimens containing methotrexate with or without adalimumab is an effective maintenance therapy in patients after an initial response is confirmed. Disease recurrence in patients on and off immunosuppression support need for ongoing radiologic surveillance regardless of immunosuppression regimen.
Keywords: immunosuppression; sarcoidosis; ventricular arrhythmia.
Figures
References
-
- Kandolin R, Lehtonen J, Airaksinen J, Vihinen T, Miettinen H, Ylitalo K, Kaikkonen K, Tuohinen S, Haataja P, Kerola T, Kokkonen J, Pelkonen M, Pietila‐Effati P, Utrianen S, Kupari M. Cardiac sarcoidosis: epidemiology, characteristics, and outcome over 25 years in a nationwide study. Circulation. 2015;131:624–632. - PubMed
-
- Roberts WC, McAllister HA, Ferrans VJ. Sarcoidosis of heart—clinicopathologic study of 35 necropsy patients and review of 78 previously described necropsy patients. Am J Med. 1977;63:86–108. - PubMed
-
- Nery PB, Mc Ardle BA, Redpath CJ, Leung E, Lemery R, Dekemp R, Yang J, Keren A, Beanlands RS, Birnie DH. Prevalence of cardiac sarcoidosis in patients presenting with monomorphic ventricular tachycardia. Pacing Clin Electrophysiol. 2014;37:364–374. - PubMed
-
- Nagai T, Nagano N, Sugano Y, Asaumi Y, Aiba T, Kanzaki H, Kusano K, Noguchi T, Yasuda S, Ogawa H, Anzai T. Effect of corticosteroid therapy on long‐term clinical outcome and left ventricular function in patients with cardiac sarcoidosis. Circ J. 2015;79:1593–1600. - PubMed
-
- Mc Ardle BA, Birnie DH, Klein R, de Kemp RA, Leung E, Renaud J, DaSilva J, Wells GA, Beanlands RS, Nery PB. Is there an association between clinical presentation and the location and extent of myocardial involvement of cardiac sarcoidosis as assessed by (1)(8)F‐fluorodoexyglucose positron emission tomography? Circ Cardiovasc Imaging. 2013;6:617–626. - PubMed
