

Functional Deficits in the Less-Impaired Arm of Stroke Survivors Depend on Hemisphere of Damage and Extent of Paretic Arm Impairment
- PMID: 31538852
- PMCID: PMC6954970
- DOI: 10.1177/1545968319875951
Functional Deficits in the Less-Impaired Arm of Stroke Survivors Depend on Hemisphere of Damage and Extent of Paretic Arm Impairment
Abstract
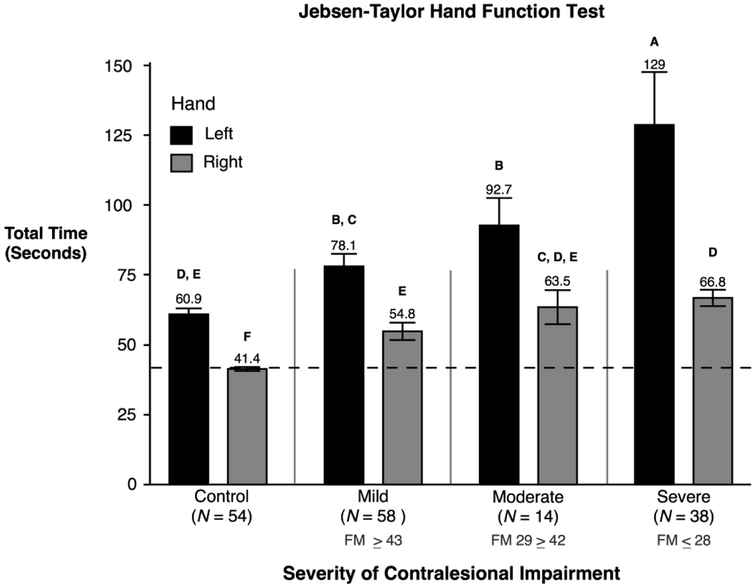
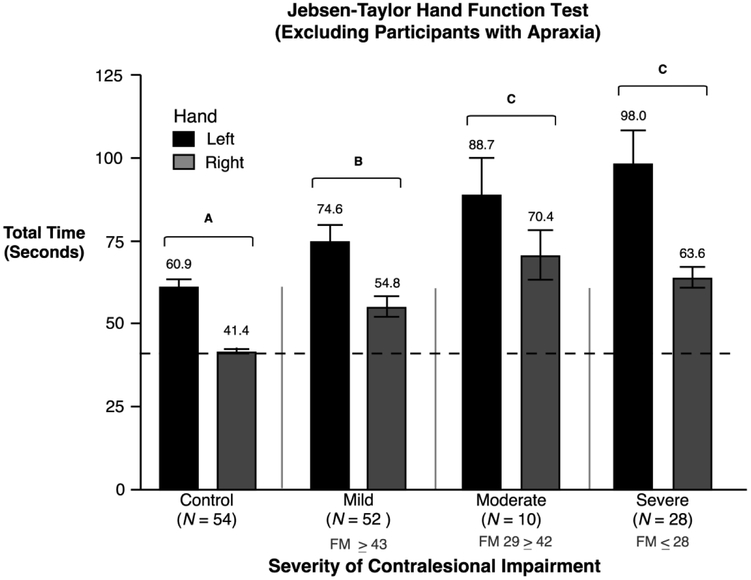
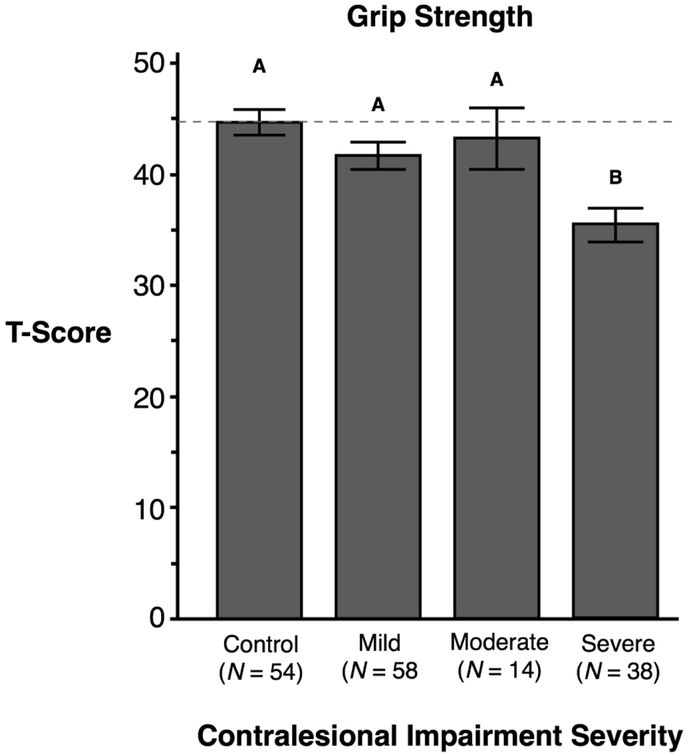
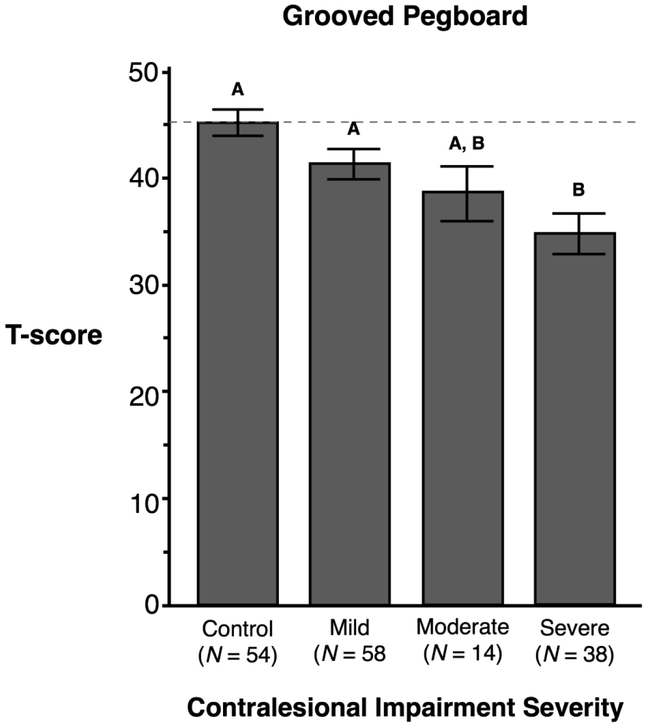
Background. Previous research has detailed the hemisphere dependence and specific kinematic deficits observed for the less-affected arm of patients with unilateral stroke. Objective. We now examine whether functional motor deficits in the less-affected arm, measured by standardized clinical measures of motor function, also depend on the hemisphere that was damaged and on the severity of contralesional impairment. Methods. We recruited 48 left-hemisphere-damaged (LHD) participants, 62 right-hemisphere-damaged participants, and 54 age-matched control participants. Measures of motor function included the following: (1) Jebsen-Taylor Hand Function Test (JHFT), (2) Grooved Pegboard Test (GPT), and (3) grip strength. We measured the extent of contralesional arm impairment with the upper-extremity component of the Fugl-Meyer (UEFM) assessment of motor impairment. Results. Ipsilesional limb functional performance deficits (JHFT) varied with both the damaged hemisphere and severity of contralesional arm impairment, with the most severe deficits expressed in LHD participants with severe contralesional impairment (UEFM). GPT and grip strength varied with severity of contralesional impairment but not with hemisphere. Conclusions. Stroke survivors with the most severe paretic arm impairment, who must rely on their ipsilesional arm for performing daily activities, have the greatest motor deficit in the less-affected arm. We recommend remediation of this arm to improve functional independence in this group of stroke patients.
Keywords: functional deficits; hemisphere-specific deficits; ipsilesional deficits; motor lateralization; stroke.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Figures
References
-
- Wyke M. Effect of brain lesions on the rapidity of arm movement. Neurology. 1967;17:1113–1120. - PubMed
-
- Arya KN, Pandian S, Kumar D. Task-based mirror therapy enhances ipsilesional motor functions in stroke: A pilot study. J. Bodyw. Mov. Ther 2017. - PubMed
-
- Bustrén EL, Sunnerhagen KS, Alt Murphy M. Movement Kinematics of the Ipsilesional Upper Extremity in Persons with Moderate or Mild Stroke. Neurorehabil. Neural Repair 2017. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
