

Telemonitoring of Crohn's Disease and Ulcerative Colitis (TECCU): Cost-Effectiveness Analysis
- PMID: 31538948
- PMCID: PMC6754696
- DOI: 10.2196/15505
Telemonitoring of Crohn's Disease and Ulcerative Colitis (TECCU): Cost-Effectiveness Analysis
Abstract
Background: Although electronic health interventions are considered safe and efficient, evidence regarding the cost-effectiveness of telemonitoring in inflammatory bowel disease is lacking.
Objective: We aimed to evaluate the cost-effectiveness and cost-utility of the Telemonitorización de la Enfermedad de Crohn y Colitis Ulcerosa (Telemonitoring of Crohn's Disease and Ulcerative Colitis [TECCU]) Web platform (G_TECCU intervention group) for telemonitoring complex inflammatory bowel disease, compared with standard care (G_control) and nurse-assisted telephone care (G_NT intervention group).
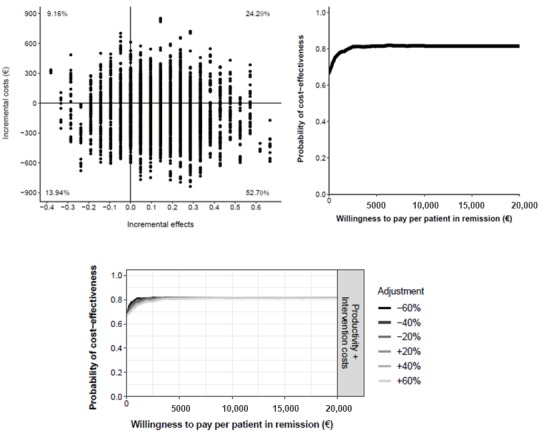
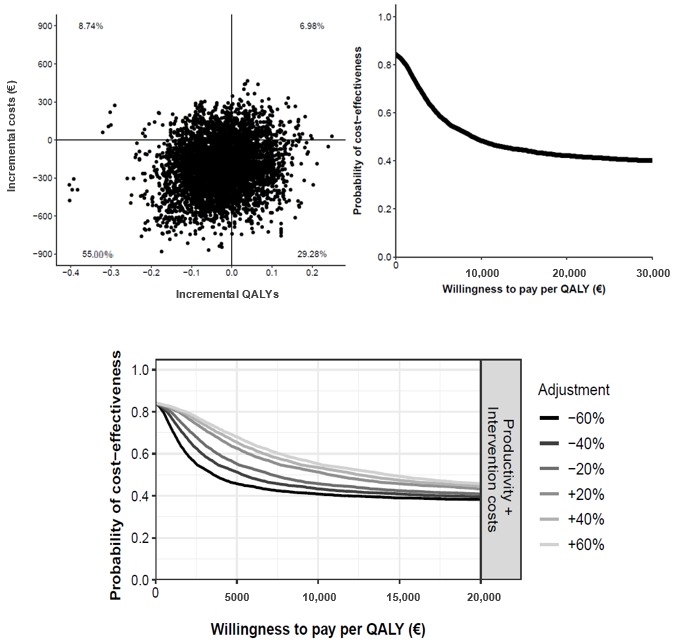
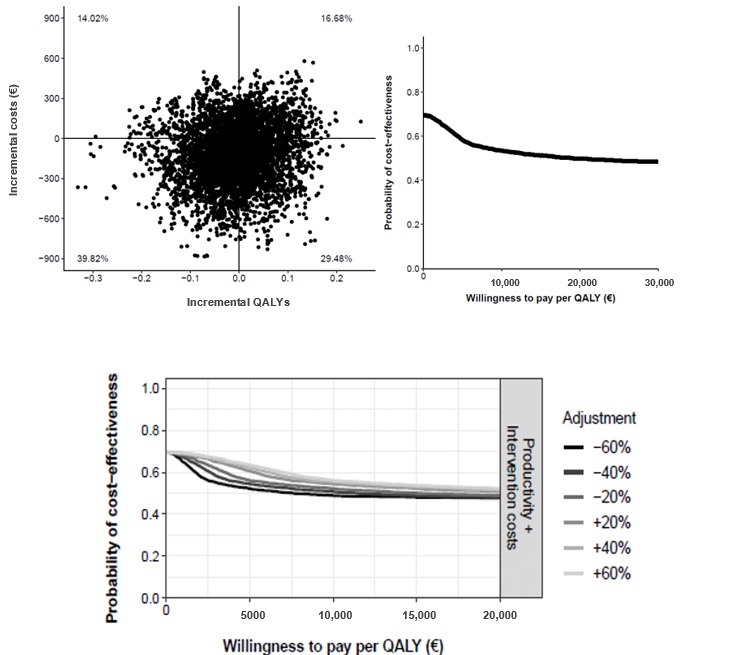
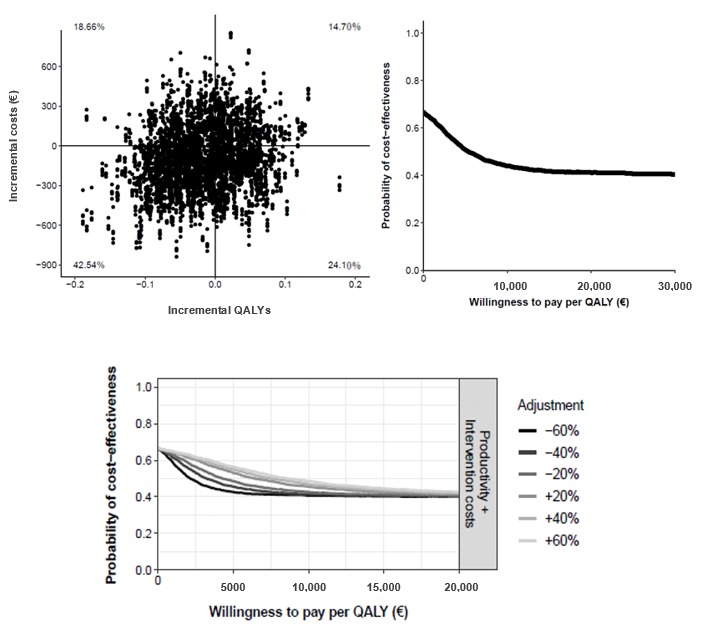
Methods: We analyzed cost-effectiveness from a societal perspective by comparing the 3 follow-up methods used in a previous 24-week randomized controlled trial, conducted at a tertiary university hospital in Spain. Patients with inflammatory bowel disease who initiated immunosuppressants or biologic agents, or both, to control inflammatory activity were recruited consecutively. Data on the effects on disease activity (using clinical indexes) and quality-adjusted life-years (using the EuroQol 5 dimensions questionnaire) were collected. We calculated the costs of health care, equipment, and patients' productivity and social activity impairment. We compared the mean costs per patient, utilities, and bootstrapped differences.
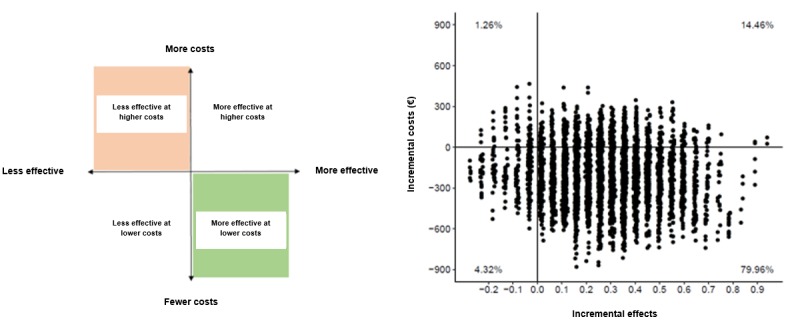
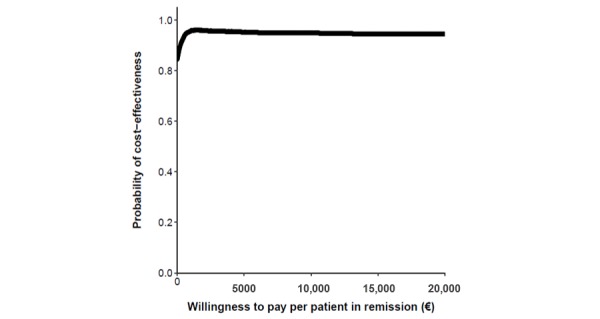
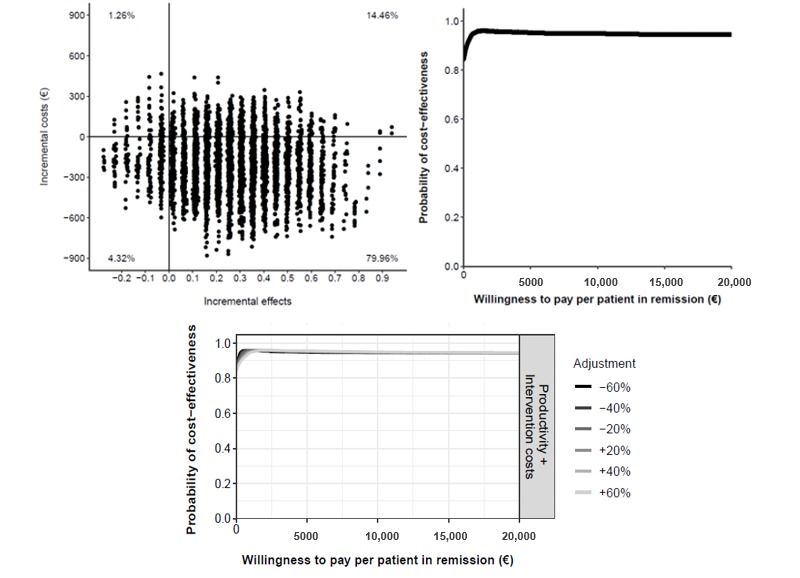
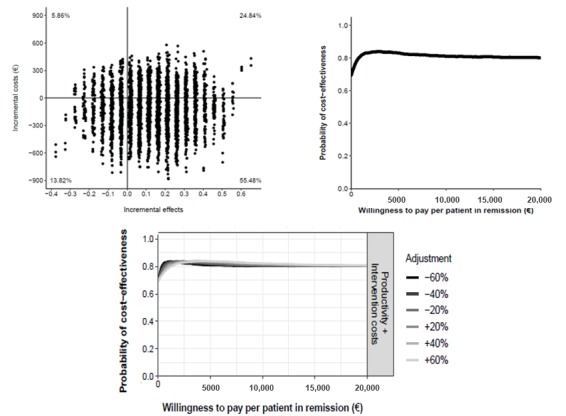
Results: We included 63 patients (21 patients per group). TECCU saved €1005 (US $1100) per additional patient in remission compared with G_control (95% CI €-13,518 to 3137; US $-14,798 to 3434), with a 79.96% probability of being more effective at lower costs. Compared with G_NT, TECCU saved €2250 (US $2463) per additional patient in remission (95% CI €-15,363 to 11,086; US $-16,817 to 12,135), and G_NT saved €538 (US $589) compared with G_control (95% CI €-6475 to 5303; US $-7088 to 5805). G_TECCU and G_NT showed an 84% and 67% probability, respectively, of producing a cost saving per additional quality-adjusted life-year (QALY) compared with G_control, considering those simulations that involved negative incremental QALYs as well.
Conclusions: There is a high probability that the TECCU Web platform is more cost-effective than standard and telephone care in the short term. Further research considering larger cohorts and longer time horizons is required.
Trial registration: ClinicalTrials.gov NCT02943538; https://clinicaltrials.gov/ct2/show/NCT02943538 (http://www. webcitation.org/746CRRtDN).
Keywords: Crohn disease; colitis, ulcerative; cost-effectiveness; eHealth; inflammatory bowel diseases; telemedicine.
©Javier Del Hoyo, Pilar Nos, Guillermo Bastida, Raquel Faubel, Diana Muñoz, Alejandro Garrido-Marín, Elena Valero-Pérez, Sergio Bejar-Serrano, Mariam Aguas. Originally published in the Journal of Medical Internet Research (http://www.jmir.org), 13.09.2019.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
References
-
- Burisch J, Jess T, Martinato M, Lakatos PL, ECCO -EpiCom The burden of inflammatory bowel disease in Europe. J Crohns Colitis. 2013 May;7(4):322–37. doi: 10.1016/j.crohns.2013.01.010. https://www-scopus-com.publicaciones.umh.es/record/display.uri?eid=2-s2.... - DOI - PubMed
-
- Bähler C, Vavricka SR, Schoepfer AM, Brüngger B, Reich O. Trends in prevalence, mortality, health care utilization and health care costs of Swiss IBD patients: a claims data based study of the years 2010, 2012 and 2014. BMC Gastroenterol. 2017 Dec 02;17(1):138. doi: 10.1186/s12876-017-0681-y. https://bmcgastroenterol.biomedcentral.com/articles/10.1186/s12876-017-0... - DOI - DOI - PMC - PubMed
-
- Peery AF, Crockett SD, Murphy CC, Lund JL, Dellon ES, Williams JL, Jensen ET, Shaheen NJ, Barritt AS, Lieber SR, Kochar B, Barnes EL, Fan YC, Pate V, Galanko J, Baron TH, Sandler RS. Burden and cost of gastrointestinal, liver, and pancreatic diseases in the United States: update 2018. Gastroenterology. 2019 Dec;156(1):254–272.e11. doi: 10.1053/j.gastro.2018.08.063. - DOI - PMC - PubMed
-
- Elbert NJ, van Os-Medendorp H, van Renselaar W, Ekeland AG, Hakkaart-van Roijen L, Raat H, Nijsten TEC, Pasmans SGMA. Effectiveness and cost-effectiveness of ehealth interventions in somatic diseases: a systematic review of systematic reviews and meta-analyses. J Med Internet Res. 2014;16(4):e110. doi: 10.2196/jmir.2790. http://www.jmir.org/2014/4/e110/ - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
