

Association of Early-Stage Breast Cancer and Subsequent Chemotherapy With Risk of Atrial Fibrillation
- PMID: 31539076
- PMCID: PMC6755537
- DOI: 10.1001/jamanetworkopen.2019.11838
Association of Early-Stage Breast Cancer and Subsequent Chemotherapy With Risk of Atrial Fibrillation
Abstract
Importance: Several types of cancer have been linked to a higher risk of developing atrial fibrillation (AF). Fewer data exist regarding early-stage breast cancer (EBC), for which cardio-oncology concerns are more pertinent.
Objective: To investigate the association of EBC and subsequent chemotherapy with the risk of developing AF.
Design, setting, and participants: This was a population-based, retrospective, matched cohort study conducted in Toronto, Ontario, Canada, of 68 113 women diagnosed with EBC between April 2007 and December 2016 who were matched 1:3 to a cancer-free control group based on birth year and receipt of breast imaging. Prevalence of AF before the index date (date of EBC diagnosis) was compared between the cohorts using the McNemar test. Cumulative incidence function curves were used to describe the AF incidence. To study preexisting AF, participants were matched before exclusion for prior AF. For the remaining analyses, we excluded women with prior AF before matching. An analysis was conducted beginning 1 year after the index date (ie, excluding AF diagnoses in year 1), which we stratified by chemotherapy exposure. Multivariable cause-specific regression was used to determine the hazard ratio (HR) associated with EBC relative to the controls and the association of chemotherapy with AF in patients with EBC.
Exposures: Breast cancer and chemotherapy.
Main outcomes and measures: Incidence of AF.
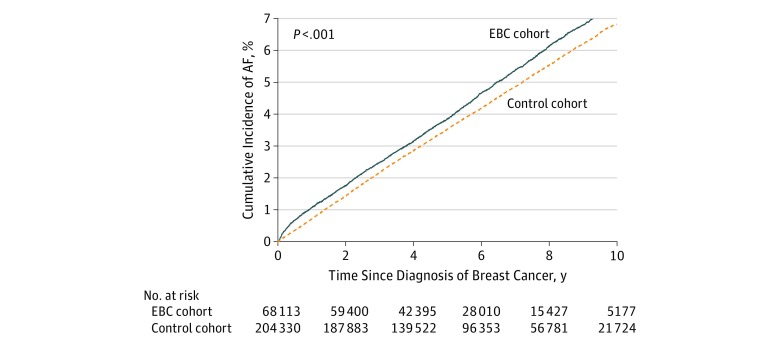
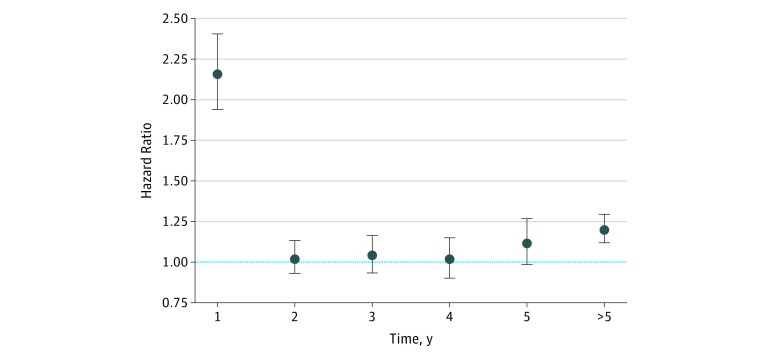
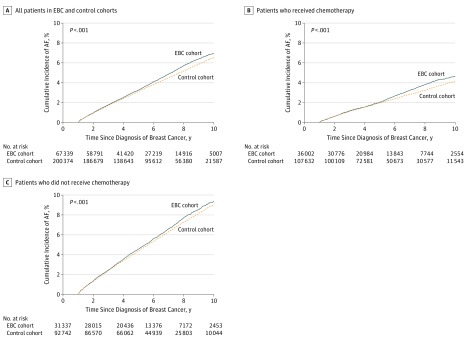
Results: A total of 68 113 women with EBC and 204 330 cancer-free controls were included in the study; both groups had a mean (SD) age of 60 (13) years. Of the women with EBC, 44.3% were diagnosed as having stage I breast cancer; 38.7%, stage II; and 13.4%, stage III; cancer stage information was missing for 3.6% of the patients. No difference was observed in preexisting AF prevalence (5.3% in the EBC cohort vs 5.2% in controls; P = .21). At 10 years after the index date, the AF incidence was 7.4% (95% CI, 7.1%-7.7%) for women with EBC and 6.8% (95% CI, 6.7%-7.0%) for the controls (P < .001). The adjusted cause-specific HR was significantly elevated at year 1 (HR, 2.16; 95% CI, 1.94-2.41) and after year 5 (HR, 1.20; 95% CI, 1.11-1.30) but not during years 2 through 5. Analyses beginning 1 year after diagnosis showed attenuated differences that remained statistically significant: the cumulative incidence of AF at 9-year follow-up was 7.0% (95% CI, 6.7%-7.3%) for patients with EBC and 6.5% (95% CI, 6.3%-6.7%) for the cancer-free controls. The rate of AF was higher in women who received chemotherapy (adjusted HR, 1.23; 95% CI, 1.13-1.35) but was not associated with exposure to anthracyclines or trastuzumab.
Conclusions and relevance: This study's findings suggest that patients with EBC may not have a higher prevalence of AF before cancer diagnosis. A higher rate of AF was observed in the first year and after 5 years following the EBC diagnosis. The rate of AF was higher in patients who received chemotherapy but appeared to not be associated with specific cardiotoxic agents. These findings suggest that the early and late periods of increased AF risk in EBC survivors warrant focused research to better understand the underlying causes and subsequent implications.
Conflict of interest statement
Figures
Similar articles
-
The Risk of Heart Failure and Other Cardiovascular Hospitalizations After Early Stage Breast Cancer: A Matched Cohort Study.J Natl Cancer Inst. 2019 Aug 1;111(8):854-862. doi: 10.1093/jnci/djy218. J Natl Cancer Inst. 2019. PMID: 30715404 Free PMC article.
-
Characteristics and Outcomes of Women Developing Heart Failure After Early Stage Breast Cancer Chemotherapy: A Population-Based Matched Cohort Study.Circ Heart Fail. 2021 Jul;14(7):e008110. doi: 10.1161/CIRCHEARTFAILURE.120.008110. Epub 2021 Jun 30. Circ Heart Fail. 2021. PMID: 34187164 Free PMC article.
-
Association of Surgical Left Atrial Appendage Occlusion With Subsequent Stroke and Mortality Among Patients Undergoing Cardiac Surgery.JAMA. 2018 May 22;319(20):2116-2126. doi: 10.1001/jama.2018.6024. JAMA. 2018. PMID: 29800182 Free PMC article.
-
The incidence of atrial fibrillation with trastuzumab treatment: A systematic review and meta-analysis.Cardiovasc Ther. 2018 Dec;36(6):e12475. doi: 10.1111/1755-5922.12475. Epub 2018 Nov 28. Cardiovasc Ther. 2018. PMID: 30372591
-
Adjuvant chemotherapy in elderly patients with early breast cancer. Impact of age and comprehensive geriatric assessment on tumor board proposals.Crit Rev Oncol Hematol. 2011 Aug;79(2):196-204. doi: 10.1016/j.critrevonc.2010.06.005. Epub 2010 Jul 23. Crit Rev Oncol Hematol. 2011. PMID: 20655243 Review.
Cited by
-
Hemorrhage Risk Among Patients With Breast Cancer Receiving Concurrent Direct Oral Anticoagulants With Tamoxifen vs Aromatase Inhibitors.JAMA Netw Open. 2022 Jun 1;5(6):e2219128. doi: 10.1001/jamanetworkopen.2022.19128. JAMA Netw Open. 2022. PMID: 35763294 Free PMC article.
-
Subsequent primary cancer risk and mortality among premenopausal breast cancer survivors.Sci Rep. 2025 Mar 28;15(1):10829. doi: 10.1038/s41598-024-84606-7. Sci Rep. 2025. PMID: 40155641 Free PMC article.
-
Breast Cancer and Atrial Fibrillation.J Clin Med. 2022 Mar 4;11(5):1417. doi: 10.3390/jcm11051417. J Clin Med. 2022. PMID: 35268508 Free PMC article. Review.
-
Causal associations between atrial fibrillation and breast cancer: A bidirectional Mendelian randomization analysis.Cancer Med. 2024 Mar;13(5):e7067. doi: 10.1002/cam4.7067. Cancer Med. 2024. PMID: 38468558 Free PMC article.
-
Identification of atrial fibrillation-related genes through transcriptome data analysis and Mendelian randomization.Front Cardiovasc Med. 2024 Jul 11;11:1414974. doi: 10.3389/fcvm.2024.1414974. eCollection 2024. Front Cardiovasc Med. 2024. PMID: 39055656 Free PMC article.
References
-
- Mehta LS, Watson KE, Barac A, et al. ; American Heart Association Cardiovascular Disease in Women and Special Populations Committee of the Council on Clinical Cardiology; Council on Cardiovascular and Stroke Nursing; and Council on Quality of Care and Outcomes Research . Cardiovascular disease and breast cancer: where these entities intersect: a scientific statement from the American Heart Association. Circulation. 2018;137(8):e30-e66. doi:10.1161/CIR.0000000000000556 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
