

Current Clinical Strategies of Pancreatic Cancer Treatment and Open Molecular Questions
- PMID: 31540286
- PMCID: PMC6770743
- DOI: 10.3390/ijms20184543
Current Clinical Strategies of Pancreatic Cancer Treatment and Open Molecular Questions
Abstract
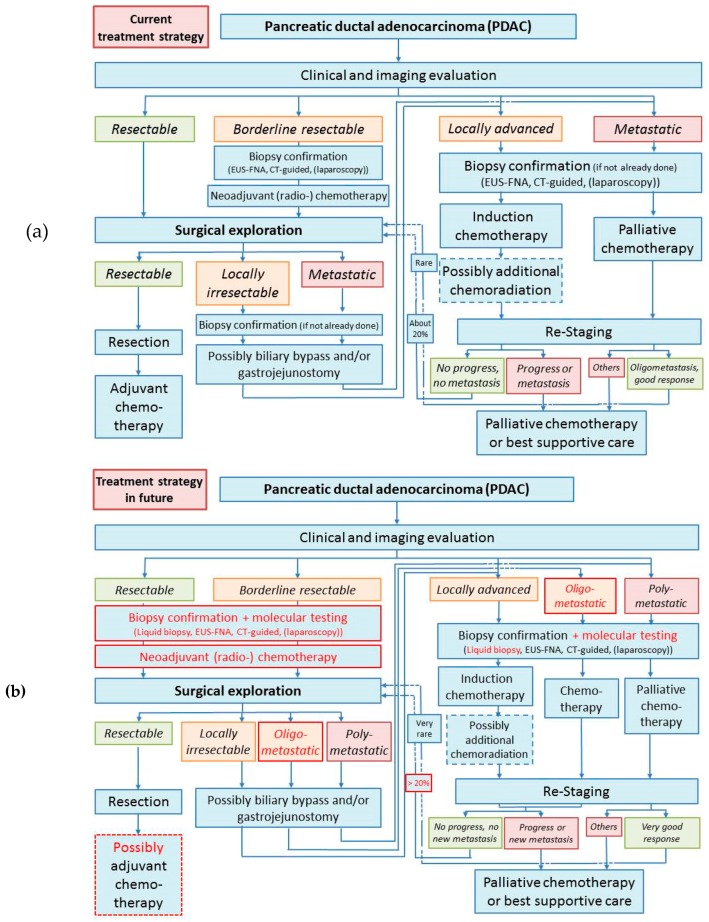
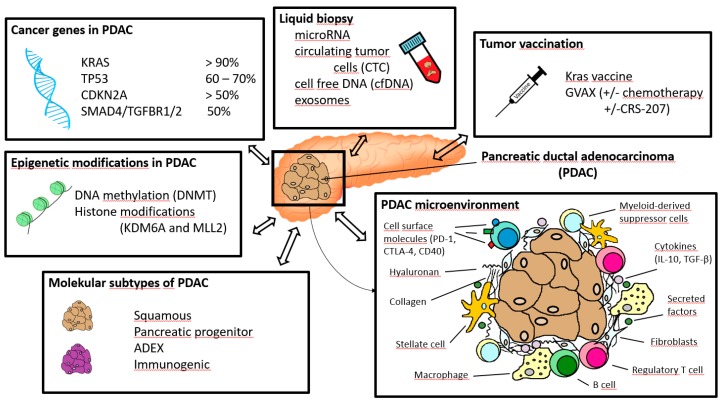
Pancreatic cancer is one of the most lethal malignancies and is associated with a poor prognosis. Surgery is considered the only potential curative treatment for pancreatic cancer, followed by adjuvant chemotherapy, but surgery is reserved for the minority of patients with non-metastatic resectable tumors. In the future, neoadjuvant treatment strategies based on molecular testing of tumor biopsies may increase the amount of patients becoming eligible for surgery. In the context of non-metastatic disease, patients with resectable or borderline resectable pancreatic carcinoma might benefit from neoadjuvant chemo- or chemoradiotherapy followed by surgeryPatients with locally advanced or (oligo-/poly-)metastatic tumors presenting significant response to (neoadjuvant) chemotherapy should undergo surgery if R0 resection seems to be achievable. New immunotherapeutic strategies to induce potent immune response to the tumors and investigation in molecular mechanisms driving tumorigenesis of pancreatic cancer may provide novel therapeutic opportunities in patients with pancreatic carcinoma and help patient selection for optimal treatment.
Keywords: chemoradiation; chemotherapy; immunotherapy; molecular mechanism; pancreatic cancer; surgery; therapeutic targets; treatment options.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
