

Sleep reductions associated with illicit opioid use and clinic-hour changes during opioid agonist treatment for opioid dependence: Measurement by electronic diary and actigraphy
- PMID: 31540611
- PMCID: PMC6756187
- DOI: 10.1016/j.jsat.2019.08.011
Sleep reductions associated with illicit opioid use and clinic-hour changes during opioid agonist treatment for opioid dependence: Measurement by electronic diary and actigraphy
Abstract
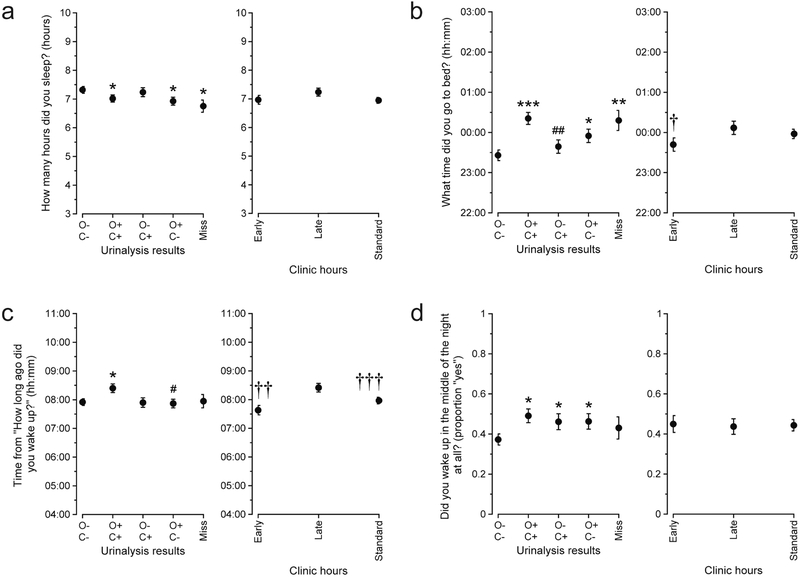
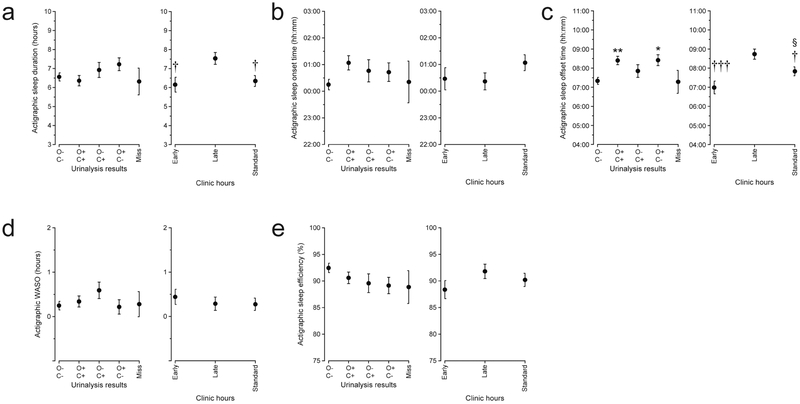
Sleep problems are commonly reported during opioid agonist treatment (OAT) for opioid use disorders. Inpatient studies have found both sleep disturbances and improved sleep during OAT. Illicit opioids can also disrupt sleep, but it is unclear how they affect sleep in outpatients receiving OAT. Therefore, we used electronic diary entries and actigraphy to measure sleep duration and timing in opioid-dependent participants (n = 37) treated with methadone (n = 15) or buprenorphine (n = 22). For 16 weeks, participants were assigned to attend our clinic under different operating hours in a crossover design: Early hours (07:00-09:00) vs. Late hours (12:00-13:00) for 4 weeks each in randomized order, followed for all participants by our Standard clinic hours (07:00-11:30) for 8 weeks. Throughout, participants made daily electronic diary self-reports of their sleep upon waking; they also wore a wrist actigraph for 6 nights in each of the three clinic-hour conditions. Drug use was assessed by thrice-weekly urinalysis. In linear mixed models controlling for other sleep-relevant factors, sleep duration and timing differed by drug use and by clinic hours. Compared to when non-using, participants slept less, went to bed later, and woke later when using illicit opioids and/or both illicit opioids and cocaine. Participants slept less and woke earlier when assigned to the Early hours. These findings highlight the role OAT clinic schedules can play in structuring the sleep/wake cycles of OAT patients and clarify some of the circumstances under which OAT patients experience sleep disruption in daily life.
Keywords: Actigraphy; Cocaine; Ecological momentary assessment; Opioid use disorder; Sleep.
Published by Elsevier Inc.
Conflict of interest statement
Figures
Similar articles
-
Multimodal assessment of sleep in men and women during treatment for opioid use disorder.Drug Alcohol Depend. 2020 Feb 1;207:107698. doi: 10.1016/j.drugalcdep.2019.107698. Epub 2019 Nov 18. Drug Alcohol Depend. 2020. PMID: 31816489 Free PMC article.
-
Effects of methadone, buprenorphine, and naltrexone on actigraphy-based sleep-like parameters in male rhesus monkeys.Addict Behav. 2022 Dec;135:107433. doi: 10.1016/j.addbeh.2022.107433. Epub 2022 Jul 22. Addict Behav. 2022. PMID: 35901553 Free PMC article.
-
Buprenorphine treatment for hospitalized, opioid-dependent patients: a randomized clinical trial.JAMA Intern Med. 2014 Aug;174(8):1369-76. doi: 10.1001/jamainternmed.2014.2556. JAMA Intern Med. 2014. PMID: 25090173 Free PMC article. Clinical Trial.
-
Dihydrocodeine for detoxification and maintenance treatment in individuals with opiate use disorders.Cochrane Database Syst Rev. 2020 Feb 18;2(2):CD012254. doi: 10.1002/14651858.CD012254.pub2. Cochrane Database Syst Rev. 2020. PMID: 32068247 Free PMC article.
-
Depression and Outcomes of Methadone and Buprenorphine Treatment Among People with Opioid Use Disorders: A Literature Review.J Dual Diagn. 2020 Apr-Jun;16(2):191-207. doi: 10.1080/15504263.2020.1726549. Epub 2020 Feb 23. J Dual Diagn. 2020. PMID: 32089124 Review.
Cited by
-
Sleep behavior traits and associations with opioid-related adverse events: a cohort study.Sleep. 2023 Sep 8;46(9):zsad118. doi: 10.1093/sleep/zsad118. Sleep. 2023. PMID: 37075812 Free PMC article.
-
I feel good? Anhedonia might not mean "without pleasure" for people treated for opioid use disorder.J Abnorm Psychol. 2021 Jul;130(5):537-549. doi: 10.1037/abn0000674. J Abnorm Psychol. 2021. PMID: 34472889 Free PMC article.
-
Addiction treatment in the postpartum period: an opportunity for evidence-based personalized medicine.Int Rev Psychiatry. 2021 Sep;33(6):579-590. doi: 10.1080/09540261.2021.1898349. Epub 2021 Jul 8. Int Rev Psychiatry. 2021. PMID: 34238101 Free PMC article. Review.
-
Quality of life during a randomized trial of a therapeutic-workplace intervention for opioid use disorder: Web-based mobile assessments reveal effects of drug abstinence and access to paid work.Drug Alcohol Depend Rep. 2021 Dec 4;1:100011. doi: 10.1016/j.dadr.2021.100011. eCollection 2021 Dec. Drug Alcohol Depend Rep. 2021. PMID: 36843907 Free PMC article.
-
Opioids, sleep, analgesia and respiratory depression: Their convergence on Mu (μ)-opioid receptors in the parabrachial area.Front Neurosci. 2023 Apr 6;17:1134842. doi: 10.3389/fnins.2023.1134842. eCollection 2023. Front Neurosci. 2023. PMID: 37090798 Free PMC article. Review.
References
-
- Anacleto TS, Adamowicz T, Simões da Costa Pinto L, & Louzada FM (2014). School schedules affect sleep timing in children and contribute to partial sleep deprivation. Mind, Brain, and Education, 8(4), 169–174. doi: 10.1111/mbe.12057 - DOI
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
