

Influence of Mortality on Estimating the Risk of Kidney Failure in People with Stage 4 CKD
- PMID: 31540963
- PMCID: PMC6830798
- DOI: 10.1681/ASN.2019060640
Influence of Mortality on Estimating the Risk of Kidney Failure in People with Stage 4 CKD
Abstract
Background: Most kidney failure risk calculators are based on methods that censor for death. Because mortality is high in people with severe, nondialysis-dependent CKD, censoring for death may overestimate their risk of kidney failure.
Methods: Using 2002-2014 population-based laboratory and administrative data for adults with stage 4 CKD in Alberta, Canada, we analyzed the time to the earliest of kidney failure, death, or censoring, using methods that censor for death and methods that treat death as a competing event factoring in age, sex, diabetes, cardiovascular disease, eGFR, and albuminuria. Stage 4 CKD was defined as a sustained eGFR of 15-30 ml/min per 1.73 m2.
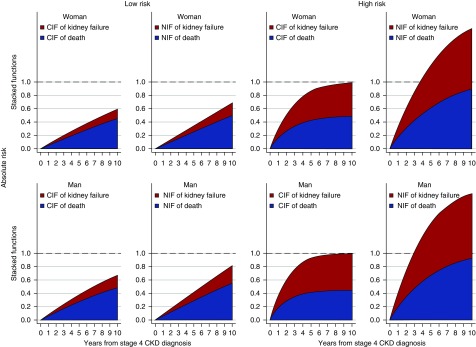
Results: Of the 30,801 participants (106,447 patient-years at risk; mean age 77 years), 18% developed kidney failure and 53% died. The observed risk of the combined end point of death or kidney failure was 64% at 5 years and 87% at 10 years. By comparison, standard risk calculators that censored for death estimated these risks to be 76% at 5 years and >100% at 7.5 years. Censoring for death increasingly overestimated the risk of kidney failure over time from 7% at 5 years to 19% at 10 years, especially in people at higher risk of death. For example, the overestimation of 5-year absolute risk ranged from 1% in a woman without diabetes, cardiovascular disease, or albuminuria and with an eGFR of 25 ml/min per 1.73 m2 (9% versus 8%), to 27% in a man with diabetes, cardiovascular disease, albuminuria >300 mg/d, and an eGFR of 20 ml/min per 1.73 m2 (78% versus 51%).
Conclusions: Kidney failure risk calculators should account for death as a competing risk to increase their accuracy and utility for patients and providers.
Keywords: Competing risks; chronic kidney disease; kidney failure.
Copyright © 2019 by the American Society of Nephrology.
Figures




Comment in
-
Competing Risk Modeling: Time to Put it in Our Standard Analytical Toolbox.J Am Soc Nephrol. 2019 Dec;30(12):2284-2286. doi: 10.1681/ASN.2019101011. Epub 2019 Nov 15. J Am Soc Nephrol. 2019. PMID: 31732615 Free PMC article. No abstract available.
References
-
- Stevens PE, Levin A; Kidney Disease: Improving Global Outcomes Chronic Kidney Disease Guideline Development Work Group Members : Evaluation and management of chronic kidney disease: Synopsis of the kidney disease: Improving global outcomes 2012 clinical practice guideline. Ann Intern Med 158: 825–830, 2013 - PubMed
-
- Matsushita K, van der Velde M, Astor BC, Woodward M, Levey AS, de Jong PE, et al.: Chronic Kidney Disease Prognosis Consortium : Association of estimated glomerular filtration rate and albuminuria with all-cause and cardiovascular mortality in general population cohorts: A collaborative meta-analysis. Lancet 375: 2073–2081, 2010 - PMC - PubMed
-
- Tonelli M, Wiebe N, James MT, Klarenbach SW, Manns BJ, Ravani P, et al.: Alberta Kidney Disease Network : A population-based cohort study defines prognoses in severe chronic kidney disease. Kidney Int 93: 1217–1226, 2018 - PubMed
-
- Demoulin N, Beguin C, Labriola L, Jadoul M: Preparing renal replacement therapy in stage 4 CKD patients referred to nephrologists: A difficult balance between futility and insufficiency. A cohort study of 386 patients followed in Brussels. Nephrol Dial Transplant 26: 220–226, 2011 - PubMed
-
- O’Hare AM, Choi AI, Bertenthal D, Bacchetti P, Garg AX, Kaufman JS, et al.: Age affects outcomes in chronic kidney disease. J Am Soc Nephrol 18: 2758–2765, 2007 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
