

PCR-based Sepsis@Quick test is superior in comparison with blood culture for identification of sepsis-causative pathogens
- PMID: 31541157
- PMCID: PMC6754458
- DOI: 10.1038/s41598-019-50150-y
PCR-based Sepsis@Quick test is superior in comparison with blood culture for identification of sepsis-causative pathogens
Abstract
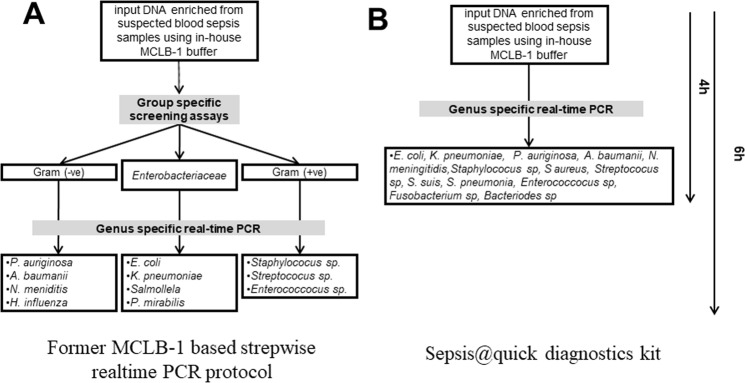
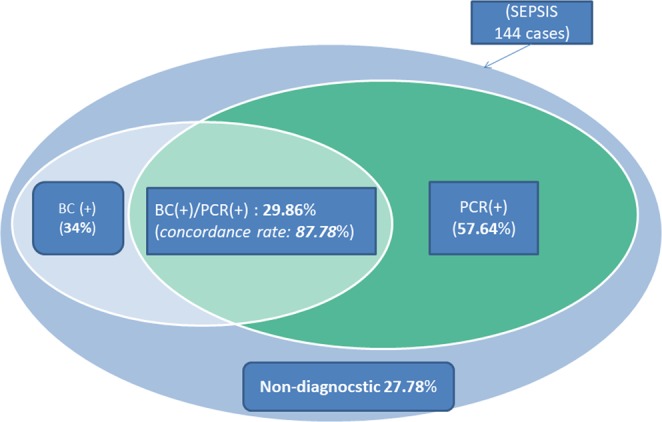
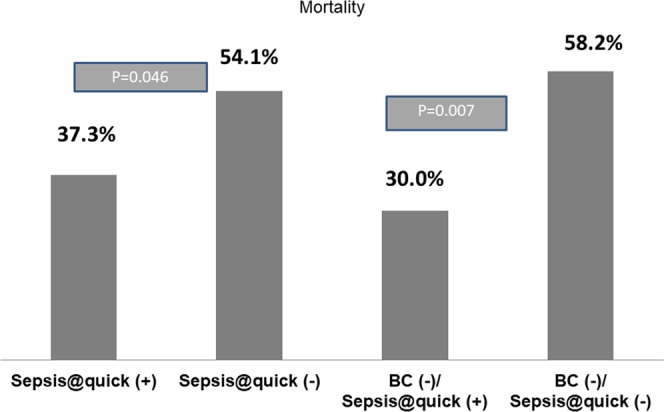
Sepsis is an acute, often fatal syndrome that requires early diagnosis and proper treatment. Blood culture (BC) is the gold standard for the identification of pathogens, however it has marked limitations, including that it is time-consuming (delaying treatment) and can only detect microbes that readily grow under culture conditions. Alternatively, non-culture-based methodologies like polymerase chain reaction (PCR) are faster but also have limitations; e.g., the reaction is often inhibited by the abundance of human DNA and thus can only detect limited known target pathogens. In our previous publication, we have demonstrated a proof-of-concept of a simple pre-analytical tool to remove human DNA from patients' blood specimens, hence allowing downstream PCRs to detect rare bacterial genetic materials. In the current study, we reported a better performance of a novel prototype diagnosis kit named Sepsis@Quick that combines human DNA removal step with real-time PCRs compared to blood-culture for identifying sepsis causative bacteria. Our data showed that Sepsis@Quick is superior to blood culture in which the novel diagnostic kit could identify more pathogens and even polymicrobial infection, faster and less influenced by the empirical administration of broad spectrum antibiotic therapy (single administration or combination of cephalosporin III and fluoroquinolon). Additionally, for the first time, we demonstrated that positive results achieved by Sepsis@Quick are significantly associated with a reduction of sepsis-related mortality.
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Herran-Monge, R. et al. Epidemiology and Changes in Mortality of Sepsis After the Implementation of Surviving Sepsis Campaign Guidelines. J Intensive Care Med. 885066617711882 (2017). - PubMed
-
- Gerdes JS. Clinicopathologic approach to the diagnosis of neonatal sepsis. Isr J Med Sci. 1994;30:430–441. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
