

Selective Intensive Care Unit Admission After Adult Supratentorial Tumor Craniotomy: Complications, Length of Stay, and Costs
- PMID: 31541243
- PMCID: PMC6911731
- DOI: 10.1093/neuros/nyz388
Selective Intensive Care Unit Admission After Adult Supratentorial Tumor Craniotomy: Complications, Length of Stay, and Costs
Abstract
Background: Admitting patients to an intensive care or medium care unit (ICU/MCU) after adult supratentorial tumor craniotomy remains common practice even though some studies have suggested lower level care is sufficient for selected patients. We have introduced a "no ICU, unless" policy for tumor craniotomy patients.
Objective: To provide a quieter postoperative environment for patients, reduce the burden on the ICU department, and to evaluate whether costs can be reduced.
Methods: A cohort study was performed comparing patients that underwent tumor craniotomy for supratentorial tumors during 1 yr after introduction (n = 109) of the new policy with the year before (n = 107). Rate of complications was evaluated, as was the length of stay and patient satisfaction using qualitative evaluation. Finally, costs were evaluated comparing the situation before and after implementation of the new protocol.
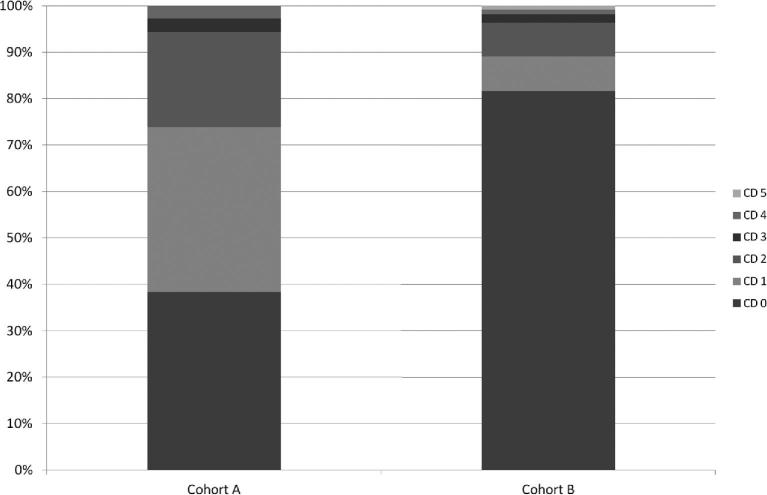
Results: A reduction in ICU/MCU admittance from 64% to 24% of patients was found resulting in 13.3% cost reduction (€1950 per case), without increasing the length of stay at the ward. The length of stay in the hospital was similar. Complications were significantly reduced after implementing the new policy (0.98 vs 0.53 per patient, P = .003). Patients that were interviewed after the new policy reported feeling safe and at ease at the ward.
Conclusion: Changing our policy from "ICU, unless" to "no ICU, unless" reduced complication rates and length of stay in the hospital while keeping patients satisfied. Hospital costs related to the admission have been significantly reduced by the new policy.
Keywords: Brain tumor; Healthcare costs; Neurosurgery; Postoperative care; Quality improvement.
© Congress of Neurological Surgeons 2019.
Figures
Comment in
-
Commentary: Selective Intensive Care Unit Admission After Adult Supratentorial Tumor Craniotomy: Complications, Length of Stay, and Costs.Neurosurgery. 2020 Jan 1;86(1):E62-E63. doi: 10.1093/neuros/nyz453. Neurosurgery. 2020. PMID: 31642508 No abstract available.
-
Commentary: Selective Intensive Care Unit Admission After Adult Supratentorial Tumor Craniotomy: Complications, Length of Stay, and Costs.Neurosurgery. 2020 Jan 1;86(1):E60-E61. doi: 10.1093/neuros/nyz427. Neurosurgery. 2020. PMID: 31670369 No abstract available.
-
In Reply: Selective Intensive Care Unit Admission After Adult Supratentorial Tumor Craniotomy: Complications, Length of Stay, and Costs.Neurosurgery. 2020 Jun 1;86(6):E574. doi: 10.1093/neuros/nyaa018. Neurosurgery. 2020. PMID: 31996910 Free PMC article. No abstract available.
-
Letter: Selective Intensive Care Unit Admission After Adult Supratentorial Tumor Craniotomy: Complications, Length of Stay, and Costs.Neurosurgery. 2020 Jun 1;86(6):E572-E573. doi: 10.1093/neuros/nyaa016. Neurosurgery. 2020. PMID: 31996916 No abstract available.
References
-
- Ziai WC, Varelas PN, Zeger SL, Mirski MA, Ulatowski JA. Neurologic intensive care resource use after brain tumor surgery: an analysis of indications and alternative strategies. Crit Care Med. 2003;31(12):2782-2787. - PubMed
-
- de Almeida CC, Boone MD, Laviv Y, Kasper BS, Chen CC, Kasper EM. The utility of routine intensive care admission for patients undergoing intracranial neurosurgical procedures: a systematic review. Neurocrit Care. 2018;28(1):35-42. - PubMed
-
- Kelly DF. Neurosurgical postoperative care. Neurosurg Clin N Am 1994;5(4):789-810. - PubMed
-
- Taylor WA, Thomas NW, Wellings JA, Bell BA. Timing of postoperative intracranial hematoma development and implications for the best use of neurosurgical intensive care. J Neurosurg. 1995;82(1):48-50. - PubMed
-
- Lonjaret L, Guyonnet M, Berard E et al.. Postoperative complications after craniotomy for brain tumor surgery. Anaesth Crit Care Pain Med. 2017;36(4):213-218. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
