

In-Hospital Mortality in Patients with Idiopathic Pulmonary Fibrosis: A US Cohort Study
- PMID: 31541276
- PMCID: PMC6861436
- DOI: 10.1007/s00408-019-00270-z
In-Hospital Mortality in Patients with Idiopathic Pulmonary Fibrosis: A US Cohort Study
Abstract
Purpose: In patients with idiopathic pulmonary fibrosis (IPF), hospitalizations are associated with high mortality. We sought to determine in-hospital mortality rates and factors associated with in-hospital mortality in patients with IPF.
Methods: Patients with IPF were identified from the Premier Healthcare Database, a representative administrative dataset that includes > 20% of hospital discharges in the US, using an algorithm based on diagnostic codes and billing data. We used logistic regression to analyze associations between patient-, hospital-, and treatment-related characteristics and a composite primary outcome of death during the index visit, lung transplant during the index visit and > 1 day after admission, or death during a readmission within 90 days.
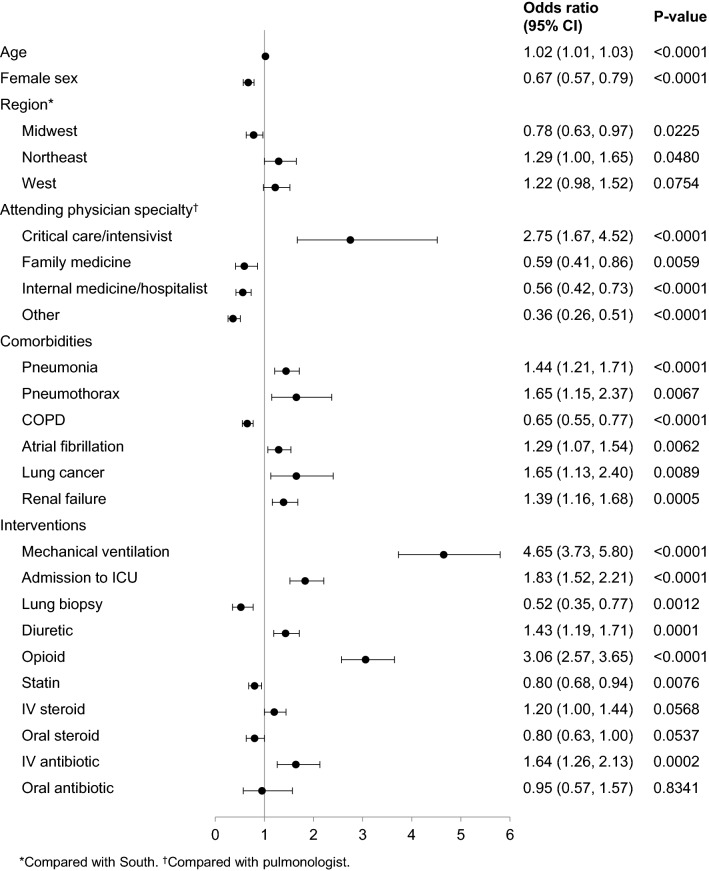
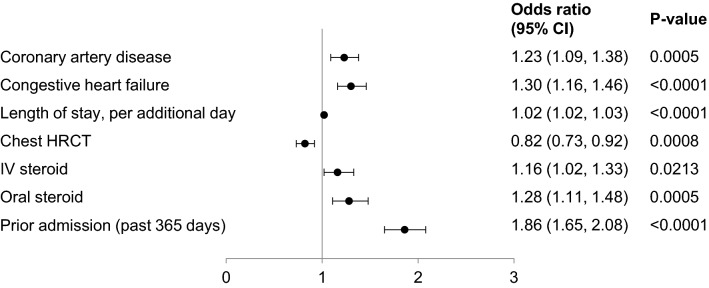
Results: The cohort comprised 6665 patients with IPF hospitalized between October 2011 and October 2014. A total of 963 (14.4%) met the primary outcome. Factors significantly associated with a higher risk of the primary outcome included mechanical ventilation [odds ratio 4.65 (95% CI 3.73, 5.80)], admission to the intensive care unit [1.83 (1.52, 2.21)], treatment with opioids (3.06 [2.57, 3.65]), and a diagnosis of pneumonia [1.44 (1.21, 1.71)]. Factors significantly associated with a lower risk included concurrent chronic obstructive pulmonary disease [0.65 (0.55, 0.77)] and female sex [0.67 (0.57, 0.79)].
Conclusions: Patients with IPF, particularly those receiving mechanical ventilation or intensive care, are at substantial risk of death or lung transplant during hospitalization or death during a readmission within 90 days.
Keywords: Critical care; Hospitalization; Intensive care; Interstitial lung disease; Mechanical ventilation.
Conflict of interest statement
MTD, OM, BRS, and SMP are faculty members in the Duke Clinical Research Institute (DCRI), which received funding from Boehringer Ingelheim Pharmaceuticals, Inc (BIPI) to coordinate this project. MTD also reports grants and personal fees from Boehringer Ingelheim, and personal fees from Roche. JL was an employee of DCRI at the time that this research was conducted. JJ, DB, and SBR are employees of Premier, Inc which received funding from BIPI for work related to this project. SB, TL, and CSC are employees of BIPI
Figures
References
-
- Raghu G, Remy-Jardin M, Myers JL, Richeldi L, Ryerson CJ, Lederer DJ, Behr J, Cottin V, Danoff SK, Morell F, Flaherty KR, Wells A, Martinez FJ, Azuma A, Bice TJ, Bouros D, Brown KK, Collard HR, Duggal A, Galvin L, Inoue Y, Jenkins RG, Johkoh T, Kazerooni EA, Kitaichi M, Knight SL, Mansour G, Nicholson AG, Pipavath SNJ, Buendía-Roldán I, Selman M, Travis WD, Walsh S, Wilson KC; American Thoracic Society, European Respiratory Society, Japanese Respiratory Society, and Latin American Thoracic Society Diagnosis of idiopathic pulmonary fibrosis. An official ATS/ERS/JRS/ALAT clinical practice guideline. Am J Respir Crit Care Med. 2018;198:e44–e68. doi: 10.1164/rccm.201807-1255ST. - DOI - PubMed
-
- Durheim M, Collard HR, Roberts RS, Brown KK, Flaherty KR, King TE, Jr, Palmer SM, Raghu G, Snyder LD, Anstrom KJ, Martinez FJ. Association of hospital admission and forced vital capacity endpoints with survival in patients with idiopathic pulmonary fibrosis: analysis of a pooled cohort from three clinical trials. Lancet Respir Med. 2015;3:388–396. doi: 10.1016/S2213-2600(15)00093-4. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
